STAPEDOTOMY (with or without LASER)
INFORMATION and SURGICAL INFORMED CONSENT
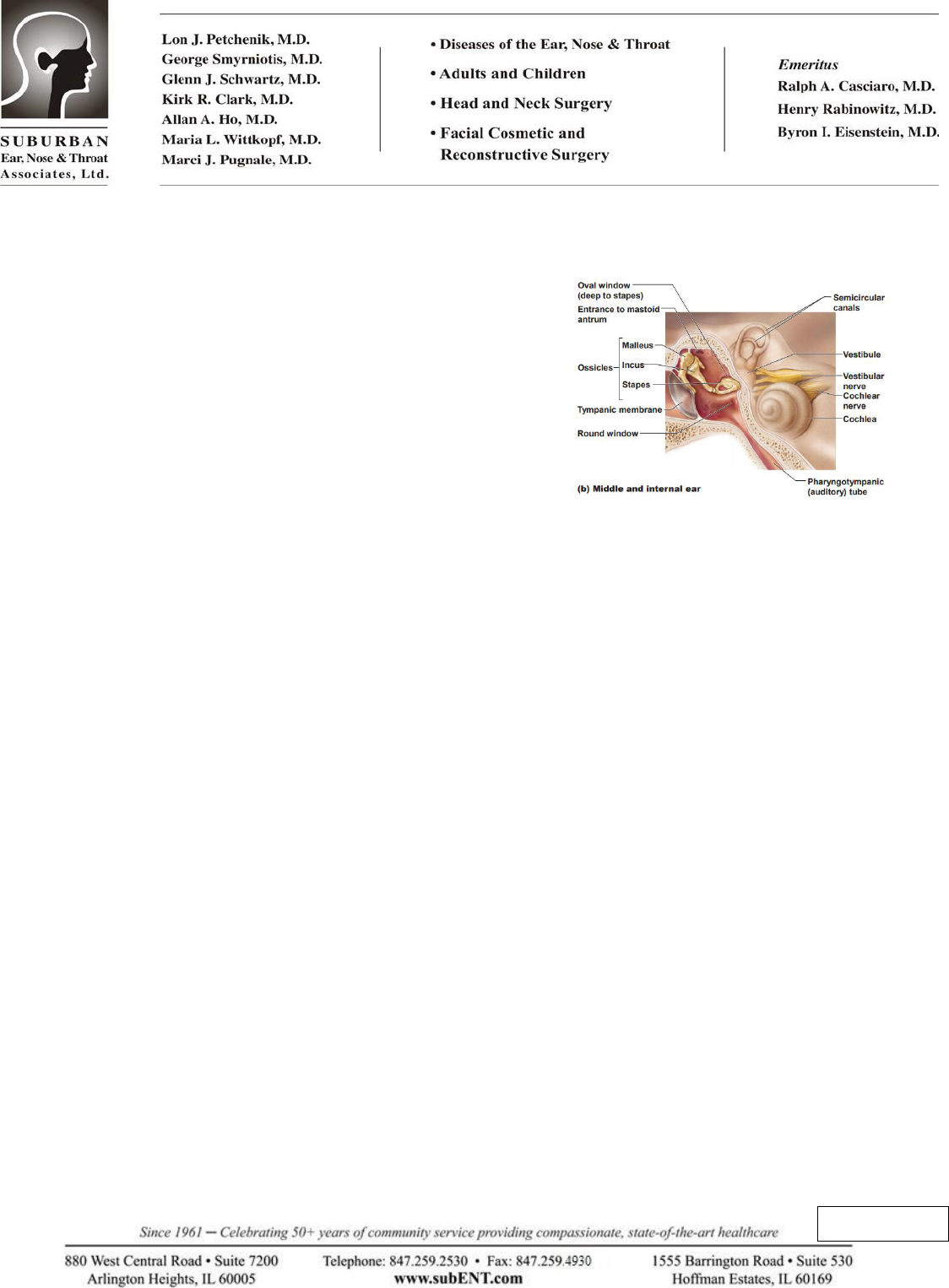
Hearing is a very complex mechanism. Sound waves enter
your ear canal where they cause the tympanic membrane
(eardrum) to vibrate. The sound energy then gets amplified and
transmitted through three small middle ear bones (ossicles) to
the inner ear organ, called the cochlea, shown as the snail
shaped structure. Lastly, the sound travels along the auditory
nerve to your brain, where it is perceived as sound.
If you have a problem with any structure in the ear before the cochlea, you will have a conductive
hearing loss. Otosclerosis is a common cause of conductive hearing loss. It is an inherited disorder that
is twice as common in women. It causes excessive stiffening of the stapes bone, the smallest bone in our
body. When movement of the stapes bone is impeded (by extra calcification in otosclerosis), a
conductive hearing loss occurs.
Otosclerosis usually presents as a gradual onset of progressive hearing loss in one or both ears. If both
ears are affected by otosclerosis, they may be affected similarly, or to different degrees or have a
different time frame. Few types of hearing loss can be surgically corrected as well as otosclerosis. A
surgical procedure, known as laser stapedotomy, can usually correct most of the hearing loss related to
otosclerosis. Generally, the operation is curative for this condition. If a patient is not a candidate for the
surgery, or does not want to have surgery performed, wearing a hearing aid is also an option.
WHAT IS A STAPEDOTOMY?
Stapedotomy is an operation that creates an opening in the stapes bone, removing the upper portion of
the bone, then replacing the piston action of the original stapes (actually bypassing) with a prosthesis.
The middle ear cavity, enclosed on the outside by the tympanic membrane and the inside by the bony
wall of the inner ear, houses the sound conduction mechanism called the ossicular chain. These three
previously mentioned ossicles are suspended from the middle ear cavity by ligaments and muscles. The
Latin names of these three little bones are the malleus (hammer), incus (anvil), and stapes (stirrup). It is
interesting to note that the translations of the Latin names of these bones hint at their combined function
in transferring sound vibrations received at the eardrum to the inner ear.
The bottom of the stapes, called the footplate, makes direct contact with the inner ear, and it is at this
point that otosclerosis interferes with the transmission of sound. In otosclerosis, there is an overgrowth
Initials: ____

Page 2 of 4
of bone around the footplate, causing the stapes bone to be fixed and unable to vibrate. Stapedotomy is
performed by bypassing the immobile stapes with an artificial piston prosthesis. A very small hole (<
0.8 mm) is created with a laser in the stapes footplate to allow for placement of the prosthesis. If you
have otosclerosis in both ears, only one ear will be operated on at a time, starting with the poorer one.
The second ear, if affected, can have the surgery performed a minimum of one year later, if desired.
Two weeks before surgery: Non-steroidal anti-inflammatory drugs (NSAID’s) should be strictly avoided
for 2 weeks prior to surgery. Medications in this family include: aspirin, ibuprofen, Advil, Motrin,
Alleve, and naproxen plus others. These medicines may increase the risk of bleeding. Also, discontinue
all homeopathic or alternative medicines such as gingko biloba or ginseng. These too, may increase
bleeding.
Night before surgery: No solid foods (that includes milk, cream, etc.) for 8 hours prior to surgery.
Typically this means no solid foods after midnight before the surgery. Small volumes of clear liquids
may be taken up to 4 hours prior to surgery. This includes water, tea, Gatorade and coffee (with NO
milk or cream).
Hospital stay: Stapedotomy is usually done as an outpatient and does not require an overnight hospital
stay. On occasion, a patient may need to stay overnight. Check with your insurance company to see if
this hospitalization is covered by your policy. A decision to admit overnight may be made after surgery
if necessary.
Lab work: If lab work is needed, it is done prior to surgery. If surgery is done as an out-patient, labs may
be obtained just after the preoperative examination. Your insurance carrier may dictate the lab where the
blood is drawn.
The indications and risks of surgery must be understood prior to proceeding with your surgery. The
alternative to this surgery is no surgery at all, which would leave your ear in its current condition.
Another option is to wear a hearing aid.
SURGICAL RISKS AND COMPLICATIONS
This type of ear surgery has very few serious risks. Complications from stapedotomy are infrequent and
typically related to the presence of uncommon variations in anatomy. Usually the surgical procedure is
performed without difficulty, with a high rate of success.
Excessive bleeding during this surgery is rare.
Post-operative infection is also rare. If this was to occur you could lose the hearing in the operated
ear. Once healed, it is unlikely that a middle ear infection would harm you.
Hearing loss: The incidence of total hearing loss reported is about one in 200 cases. Generally 90% of
patients find a significant improvement in their hearing after surgery. 5 to 10% of patients may not
experience an improvement in their hearing or a reduction in their hearing. If your hearing is not
Initials: ____

Page 3 of 4
significantly improved after the surgery, a hearing aid can be obtained. If there is loss of hearing from
the surgery, a hearing aid would not benefit you. There is also a 1% chance over the years that
delayed deafness can occur. This would most commonly occur with a significant barometric pressure
change such as on a plane flight or scuba diving.
Dizziness/Vertigo: it is not uncommon to experience dizziness or vertigo for hours or days after the
surgery. Extremely rarely the dizziness would not resolve.
Eardrum perforation: there is a small chance your eardrum may develop a hole during surgery. Repair
of this would be attempted at the surgery however if it persists a second surgery might be necessary.
Tinnitus: tinnitus that was present before the surgery commonly persists, although following surgery
it may disappear. In rare instances it could be worse.
Facial nerve paralysis: injury to the facial nerve is extremely rare in stapedotomy. If this was to
occur your face would droop, be weak or be paralyzed.
Taste change: a nerve called the chorda tympani nerve runs directly in the middle of the operative
site, overlying the bones that are surgically manipulated. This nerve controls the taste function of the
front 2/3 of the tongue on the side of the surgery. If this nerve is either intentionally divided (which is
occasionally necessary) or stretched, you may experience a metallic taste for several months following
surgery. Unless you rely on your taste buds for your profession (such as a sommelier does), one-sided
loss won’t likely have any permanent noticeable alteration of taste or flavor. Loss of this nerve
function on both sides however, may leave a noticeable reduction in taste/flavor.
Laser fire: there is a very remote risk of fire when using any laser in surgery. Precautions are taken
to avoid this problem.
As with any type of surgery, the risks of anesthesia such as drug reaction, breathing difficulties and even
death are possible. Please discuss these risks with your anesthesiologist.
GENERAL POST-OPERATIVE INSTRUCTIONS/CARE
1.
ACTIVITY: Very light activity for 2-3 weeks is recommended after your ear surgery. No excessive
bending, stooping, straining, or lifting more than 15 pounds during this time. Please avoid aggressive
blowing of your nose for one month after surgery. If your job entails a lot of bending or heavy lifting,
please notify us prior to your surgery. Ideally avoid plane flight for 6 weeks, even better for 3 months
following stapes surgery. If you are an airline pilot, sky jumper or scuba diver, please be sure to alert
your physician.
2.
DIET: You can eat a diet as you tolerate after your ear surgery.
3.
MEDICINES: You will be prescribed pain medicines and possibly oral antibiotics and/or eardrops.
Take these as directed. You may also be prescribed stool softeners. Take these as directed. Avoid
Initials: ____
Page 4 of 4
heavy straining with bowel movements for several weeks.
4.
BATHING: Generally, you may shower 24 hours after surgery. We do request you keep the ear dry
for 2-3 weeks after surgery or until instructed otherwise.
5.
Post-operative follow-up: you will be asked to return to our office 7 to 10 days after surgery. There will also be
several visits over the next 4 to 6 weeks. If first post-operative visit has not already been scheduled, please call
our office to make that appointment.
At Suburban Ear, Nose and Throat Associates, Ltd., we go to great lengths to try to help you
understand your plan of care. If at any time during your care you have questions or concerns, please
call us at 847- 259-2530.
I have been given an opportunity to ask questions about my condition, alternative forms of treatment,
risks of non-treatment, the procedures to be used and the risks and hazards involved. I have sufficient
information to give this informed consent. I understand every effort will be made to provide a positive
outcome, but there are no guarantees.
Patient name PRINTED:
Patient SIGNATURE:
Date: Time:
Witness: Date:
