
Schema Therapy for
Cluster-C
Personality Disorders
Hannie van Genderen
Remco van der wijngaart
Community Mental Health Centre Maastricht




Overview
Dag 1
• Casusconceptualisatie en diagnostiek bij cluster C
• Behandeling:
• Afhankelijke persoonlijkheidsstoornis
- Willoos Inschikkelijke
• Obsessief-compulsieve persoonlijkheidsstoornis
- Overcontroleerder
Dag 2
• Afhankelijke persoonlijkheidsstoornis
- Schuldinducerende oudermodus
• Ontwijkende persoonlijkheidsstoornis
- Ontwijkende en onthechte beschermer
- Straffende oudermodus

Overview
Dag 3
• Obsessief-compulsieve persoonlijkheidsstoornis
- Veeleisende oudermodus
• Versterken gezonde volwassene en blije kind
• Afhankelijke persoonlijkheidsstoornis
• Uiten van kwaadheid en woede
Dag 4
• Praktijktoets
• Imaginairerescripting
• Autonoom gedrag

DAG 1

Kennismaken
Ervaring met ST
Supervisie/ intervisie ST
Welke knelpunten bij het maken van de
casusconceptualisatie
(formulier en model)
© H. van Genderen
9
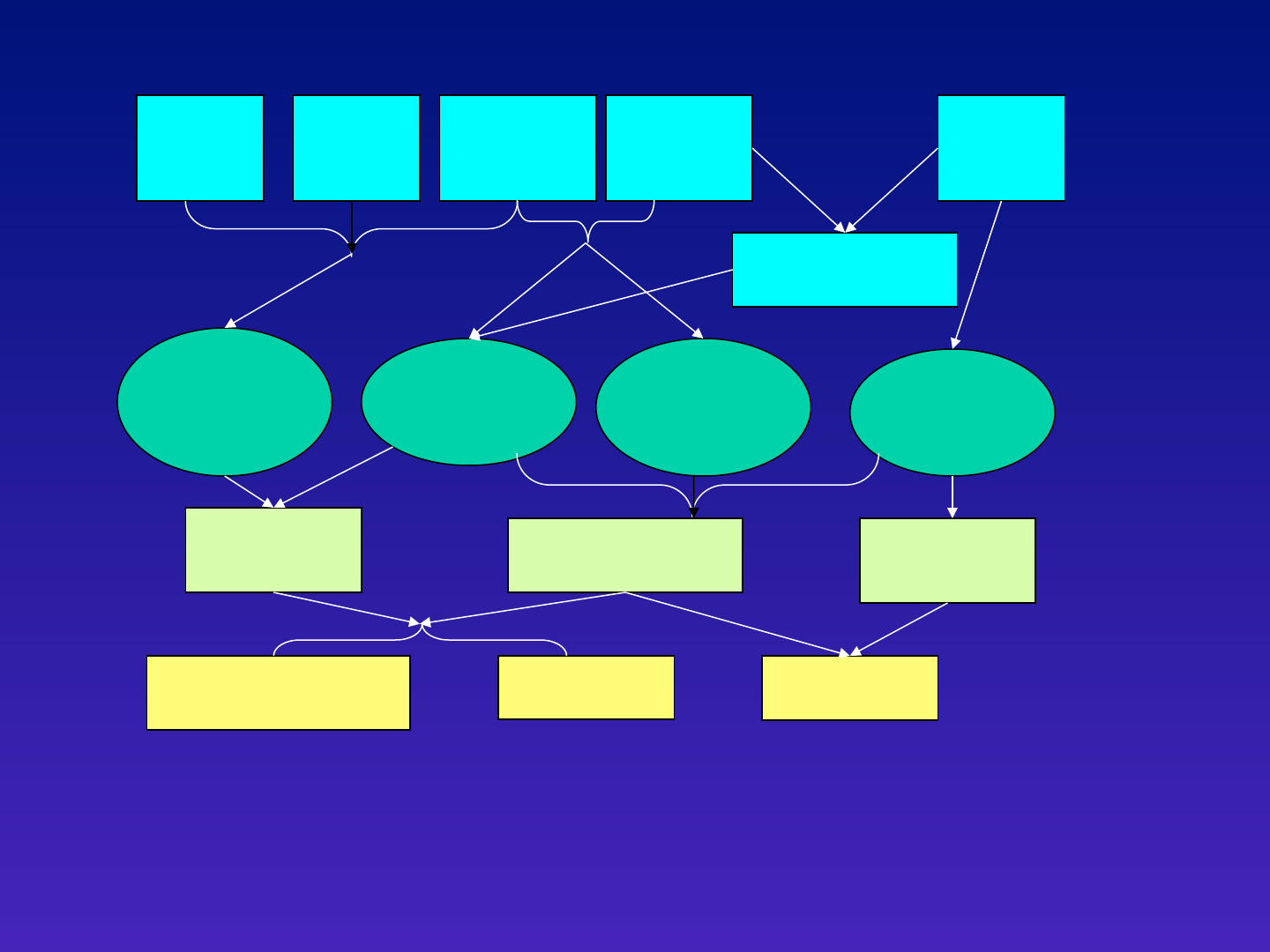
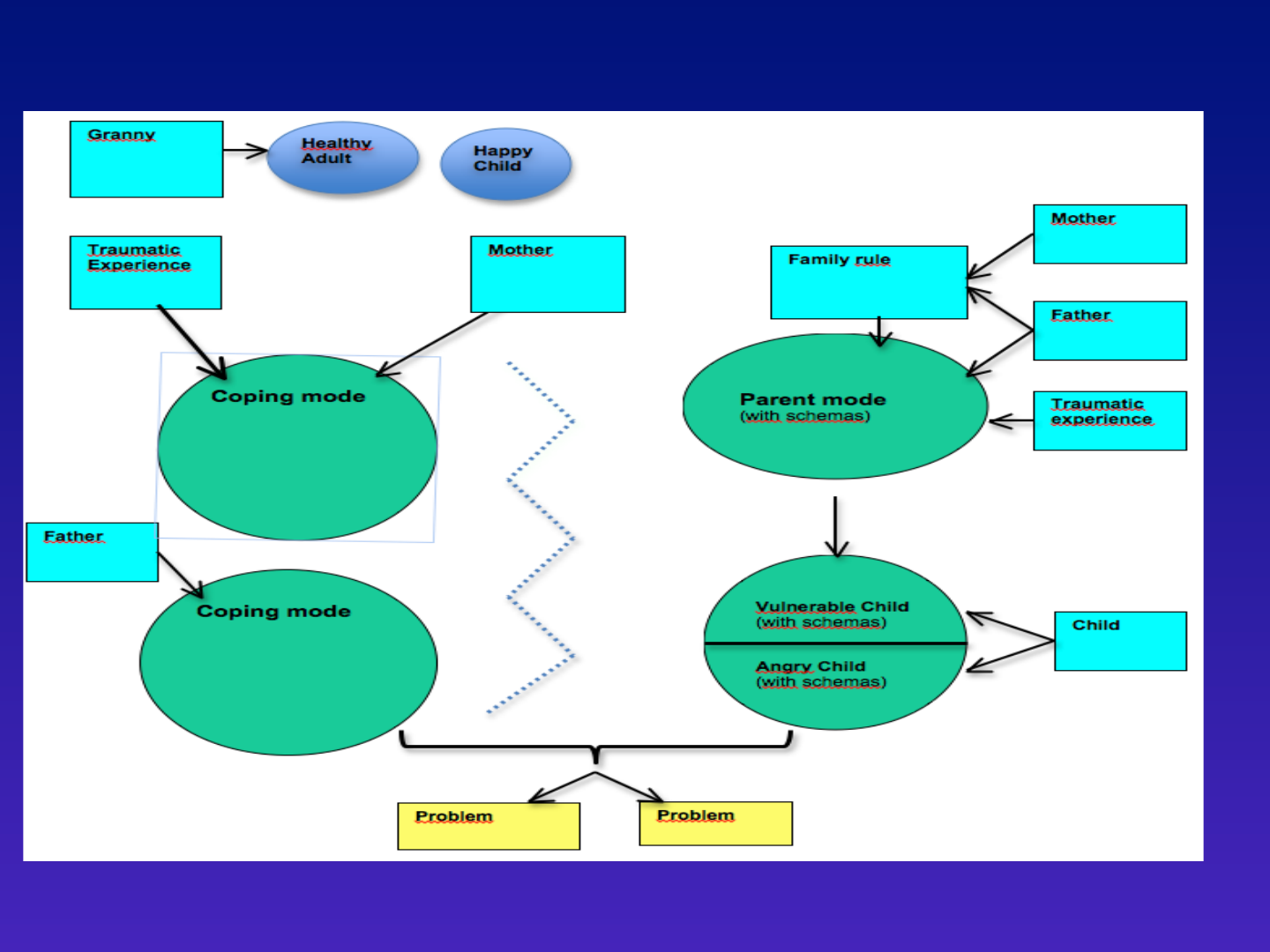
Relatieproblemen
In gezelschap angstig
en conflicten vermijden
Werkproblemen!
Ik moet voor de
ander zorgen want
die is zwakker dan ik
(zelfopoffering)
Ik ben niet belangrijk
(emotionle
verwaarlozing)
Ik ben heel anders
dan anderen (sociaal
Isolement)
Alles heel goed
willen doen
(meedeogenloze
normen)
Overgave
Altijd eerst aan
anderen denken
Vermijding
Contact met anderen
uit de weg gaan
Overgave
Altijd hard werken
en studeren
Gevoelig en
intelligent kind
Vader vaak
overspannen
Moeder zorgt
Voor vader
en broertje
Vader
veeleisend
Gezinsregel: over
gevoelens en problemen
wordt niet gepraatl
Moeder
teruggetrokken
en stil

General Conditions for
Therapy
• Check motivation for therapy, so sometimes
motivational interviewing first
• Reason for treatment can be chronic depression,
anxiety or burnout
• Explain therapy model:
- talking about the past is necessary
- changing means stop avoiding
• Pay attention to autistiform disorders
• Addiction that needs detox first

General Conditions for
Therapy
• If patiënt is not motivated to work on
PD: repeat therapy for axis I
• Explain that not working on a deeper
level can lead to chronic complaints

Research
Effect Schema Therapy compared with
treatment as usual:
• Less drop out
• More recovery
• Better social functioning (>GAF)
• Less depression
• Bamelis, L.L. M., Evers, M.A.A., Spinhoven, P. & Arntz, A. (2014). Results of a
multicentered randomized controlled trial on the clinical effectiveness of schema
therapy for personality disorders. American Journal of Psychiatry,
© H. van Genderen
13
“difficult”
parents
“difficult”
temperament
Traumas
Dysfunctional
Schemas
Dysfunctional
Coping stratgies
Complaints

Basic core needs
• Secure attachments to others (safety,
stability, nurturance and acceptance)
• Autonomy, competence and sense of
identity
• Freedom to express needs and emotions
• Spontaneity and play
• Realistic limits and self-control
Concept of a Schema Mode:
• Schema modes are moment-to-
moment emotional-cognitive states with
specific coping responses
• Similar, but more extreme to what we
all experience
• Schema modes are triggered by life
situations that we are sensitive to
• An individual may shift from one
schema mode into another (flipping)

Schema Modes
• Child modes
• Dysfunctional Coping modes
(Surrender, avoid, overcompensate)
• Dysfunctional Parent modes
• Healthy Adult mode

Unravelling the connection between
schemas, coping styles, and
modes:
empirical findings
Marleen Rijkeboer
&
Jill Lobbestael

Why did Jill and Marleen start
this project?
• Schism in schema therapy:
the schema model vs. the mode model
• Jill Lobbestael performed research into
modes. Marleen into schemas
• Both interested in:
To what extent are these two models
related?
What are the connections between the
constructs in both models?

Connecting the constructs
Adaptation of the Schema Polarity Model
by Elliott & Lassen (1997)
schema
surrender
overcompensation
avoidance
Connecting the constructs
Defectiveness/Shame
vulnerable child:
“I am unloveable”
self-aggrandizer:
“I am very special”
detached
protector
Healthy Adult “I am OK”

Connecting the constructs
Emotional Deprivation
vulnerable child:
“No-one will meet my
needs”
angry child:
“I want my needs to be
met right now”
detached
protector
healthy adult “I am respected”

The integrated model
A mediation model in which coping styles
mediate the relationship between
schemas and modes
coping style
schema schema mode

The integrated model:
another way of categorizing
modes
– Trying to connect the schema model and mode model
into a more parsimonious model
• Basically the function of moment-to-
moment states is assessed by taking
into account:
– What are the origins: the underlying theme/schema?
– What is the dominant coping style?
– We were a bit confused by the term ‘coping mode’. Isn’t
this a pleonasm? Don’t modes always involve coping?

Results
surrender
schema vulnerable child
Schemas: emotional deprivation, abandonment, mistrust,
social isolation, defectiveness, failure, vulnerability,
negativity/pessimism, functional dependence, & approval
seeking
All indirect effects were significant
Results
avoidance
schemas detached protector
Schemas: emotional deprivation, abandonment, mistrust,
social isolation, defectiveness, failure, vulnerability,
negativity/pessimism, functional dependence, emotional
inhibition & approval seeking
All indirect effects were significant
Results
overcompensation / surrender
schema angry child
Schemas: emotional deprivation, abandonment, mistrust,
social isolation, defectiveness, failure, vulnerability,
negativity/pessimism, functional dependence, emotional
inhibition & approval seeking (overcompensation)
Schemas: insufficient self-control & entitlement (surrender)
All indirect effects were significant
Results
surrender
schema punitive parent
Schemas: defectiveness, failure, punitiveness, & unrelenting
standards
All indirect effects were significant

Results
surrender/avoidance
schema compliant surrender
Schemas: approval seeking, self-sacrifice & enmeshment
(surrender)
Schemas: abandonment (avoidance)
All indirect effects were significant
Results
overcompensation / surrender
schema self-aggrandizer
Schemas: defectiveness, failure, & social isolation
(overcompensation)
Schema: entitlement (surrender)
All indirect effects were significant
Results
overcompensation
schema bully & attack
Schema: mistrust/abuse
the indirect effect was significant

Conclusion & Discussion
• Straight forward and clear relationships
between schemas, coping styles, and schema
modi were found
• Findings were cross-validated, hence results
are robust
• The schema model and the schema mode
model are closely related
• Schism of both models seems unwarranted

Emotion theory Lang
Three basic levels on which emotional
experiences are represented in memory:
• Sensory stimuli
• Meaning
• Bodily response
Therefore it’s important to use diverse
diagnostic methods!

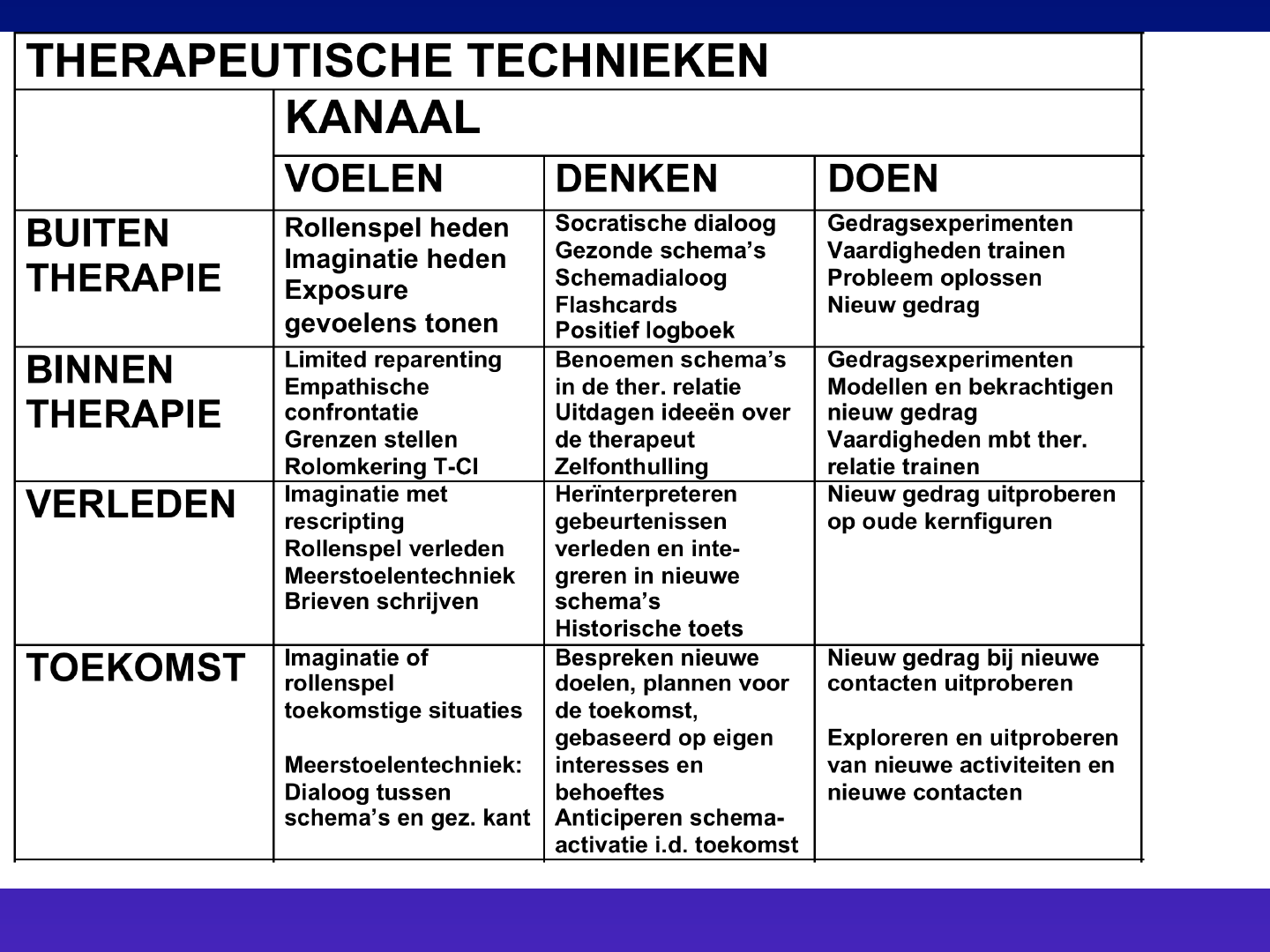
Schema Therapy
• Integrative Therapy based on the
Schema Model
• Three ways of changing schemas:
– Doing - Behavioural Techniques
– Feeling - Experiential Techniques
– Thinking - Cognitive Techniques
• Four foci:
– Therapeutic Relationship
– Experiences outside therapy
– Memories from childhood
– Future
© H. van Genderen
34
Difference between
cluster C and B
Cluster C
• Too much protection
• Emotional abuse
• Too many rules
• Deficits in parents more
“subtle”
• Punitive parent more
restrictive and guilt
inducing
• More loyalty towards
parents
• Patient quiet & obedient
• Parentification
• Not enough anger
Cluster B
• Insufficient protection
• Sexual or violent abuse
• Lack of rules
• Deficits in parents
more “obvious”
• Punitive parent more
abusive
• Loyalty towards
parents sometimes
easier to break through
• P. is not so cooperative
• Takes no responsibility
• Too much anger

Roleplay
Roleplay
about common problems
during case
conceptualisation

Protocol cluster C
• 40 sessions in year 1
– Sessions 1-6: introduction, case
conceptualization
– Sessions 7-25: focus on childhood
– Sessions 26-40: focus on present &
behavioural change
• 10 booster sessions in year 2
(+ monthly)

Protocol Session1-6
First phase of treatment
• If PD treatment is indicated and patient
agrees with Schema Therapy:
• Intake Schema Therapy, assessment of:
– Schemas, coping styles, and modes
(Discuss SMI & YSQ & Scid's)
– Origins in childhood (Life history & YPI)
– Unmet basis emotional needs
Imagery with father (alone)
Imagery with mother (alone)
– Current problems

First phase of treatment
• Link between origins, schemas, coping and
modes, and current problems
• Together with the patient: formulation of the
case conceptualization
• Explain aim and methods of the treatment
(also reading books)
• Mutual agreement and clarity on
appointments and rules
• Building a safe therapy relationship

Mode models Cluster C
• Avoidant PD
• Dependent PD
• Obsessive-Compulsive PD

AVOIDANT
& DETACHED
PROTECTOR
(& COMPLIANT
SURRENDER)
LONELY/INFERIOR
CHILD
&
ABANDONED/ABUSED
CHILD
PUNITIVE
PARENT
HEALTHY
ADULT
Avoidant PD
HAPPY
CHILD

Avoidant PD
• P. worries that he is socially inept and inferior: low
self-esteem
• P. fears that he has not the capacity to deal with
challenging situations
• Fear of novelty and emotions
• Avoids:
– Feelings (negative AND positive, especially anger)
– Experiencing bodily sensations (f.e. sexual arousal, eating
strong flavored and spicy food)
– Engaging in potentially risky activities
– Social contacts and roles
– Intimacy
– Making choices
– Having opinions and expressing them
• Emotionally abused or abandoned in childhood

Avoidant PD
• Inept and inferior: low self-esteem
• Emotionally abused or abandoned in childhood
• NEEDS:
- nurturance and acceptance
- Freedom to express needs and emotions
COMPLIANT
SURRENDER
DEPENDENT
CHILD
&
ABANDONED/ABUSED
CHILD
PUNITIVE
PARENT
(punishes
Autonomy,
Guilt inducing)
HEALTHY
ADULT
Dependent PD
HAPPY
CHILD

Dependent PD
FUNCTIONAL DEPENDENCY
EMOTIONAL DEPENDENCY
FUNCTIONAL DEPENDENCY
• Patient worries about his capacity to lead an adult life
• Cannot make minor and major decisions in a practical
sense
• Believes he has to rely on a strong person to help him
• Lack of self-confidence
• Lack of autonomy
• Authoritarian parenting

Dependent PD
EMOTIONAL DEPENDENCY
• Desperately needs somebody for emotional support
• When alone patient feels lonely and empty
• Clings to family members and friends
• Constant fear of abandonment
• Threat of abandonment in youth or parent was
dependent on the child

Dependent PD
• Believes he has to rely on a strong person to help him
• Lack of self-confidence
• Lack of autonomy
• Authoritarian parenting
• Constant fear of abandonment
NEEDS:
• Secure attachments to others (safety, stability,
nurturance and acceptance)
• Autonomy, competence and sense of identity
• Freedom to express needs and emotions

PERFECTIONISTIC
OVERCONTROLER
(denied/
not accessible)
VULNERABLE
CHILD
DEMANDING
PARENT
HEALTHY
ADULT
SELF-
AGGRANDIZER
Obs-Comp PD
HAPPY
CHILD

Obsessive-Compulsive PD
• Patient has an excessive and compulsive
devotion to productivity at the expense of
other areas of life
• Standards are usually extremely high
• Emotions are not seen as valuable
• Views himself as superior to others in terms
of conscientiousness, responsibility and moral
norms
• Emotional abuse in childhood
• Cold and strict parenting

Obsessive-Compulsive PD
• Standards are usually extremely high
• Emotions are not seen as valuable
• Emotional abuse in childhood
• Cold and strict parenting
• NEEDS:
• Secure attachments to others ( nurturance and
acceptance)
• Freedom to express needs and emotions
• Spontaneity and play

Idiosyncratic schema-mode
model
• Develop together with patient idiosyncratic
mode model
• Patient may read Young & Klosko’s self-
help book
• Adapt names of the modes
E.g., ‘the wall’, “your punishing side”
• Draw on white board
• Relate to historical roots
• Must explain present problems
Example: Dependent & OC PD
patient
Compliant Surrender
Dependent Child
PUNITIVE & DEMANDING
PARENT MODE
Perfectionistic
Overcontroller
Healthy
Adult
Happy
Child

Recognizing Schema Modes
• Feeling tone – each mode has its own
characteristic affect
• Life history
• Therapeutic relationship
• Imagery
• Questionnaires: Schema Mode Inventory

Collecting information
• Interview (life history and current
complaints)
• Questionnaires
• Imagery
• Downward-arrow

Avoidance & modes
• Detached protector
– Avoids feeling & connection (passive) incl. somatization
• Avoidant protector
– Situational avoidance
• Compliant surrender
– Avoids autonomy
• Detached self soother
– Active substance abuse & activities to avoid (active,
sensation seeking)

Recognizing different modes
at cluster C Personality
Disorder

Protocol Sessions 7-25
Second phase of treatment
• Start with asking about: Audiotape and last
week
• Identification of schemas and coping styles in
the here and now, by recognizing modes
which are present during the sessions
• Changing schemas and coping styles by
working with the modes through experiential,
cognitive, and behavioural techniques
• Processing of traumas

Protocol Sessions 7-25
• Focus on vulnerable child mode
- Sometimes directly
- Sometimes you need to address
coping mode or punitive parent
mode first
• Fight Punitive/Demanding Parent Mode
• Bypass the protector: Repeat explanation
why it will not help now
• At least once every 2 sessions
imagery rescripting

Treatment:
Content of a session
• Ask how last week went
• Examine which mode is present (don’ task)
• Choose a technique to change this mode
• Connect to the vulnerable child
• Support, and comfort the child
• Educate about needs
• Conclusions aimed at changing the schemas
and modes
• Enhance the Healthy Adult
© H. van Genderen
61

© H. van Genderen
62
Planning session in the first phase of therapy
Ask how last week went
(Don’t go into too much detail)
5
Which mode is present?
(don’t ask but name it.)
3
C
B
T
I
m
R
e
S
t
o
e
l
e
n
20-
30
Vulnerable Child
Conclusions aimed at changing the schemas
and modes. Psycho education
± 15
COMPLIANT
SURRENDER
DEPENDENT
CHILD
&
ABANDONED/ABUSED
CHILD
PUNITIVE
PARENT
(punishes
Autonomy,
Guilt inducing)
HEALTHY
ADULT
Dependent PD
HAPPY
CHILD

Treatment of Dependent PD
• Correct authoritarian parenting
• Don t allow P to submit to you and make you
an authority (mind your own schema s)
• Push to express own opinions and emotions
• Push autonomy
• Stimulate selfconfidence
• Teach how to have disagreements
• Note: this reparenting is a bit different than
with many other PDs (don t promote
dependence, but independence)

Dependent PD
• Recognizing modes
• Make contact with the vulnerable child

VULNERABLE CHILD
• Empathize with and protect the
Vulnerable Child
• Process loneliness, abuse and
abandonment
• Offer safe attachment in treatment
• Help Vulnerable Child to receive love
and care

DEPENDENT CHILD
• Note: this reparenting is a bit different
than with many other PDs
• Push to express own opinions and
emotions
• Push autonomy
• Stimulate almost any initiative to do new
things
• Set limits to not coming to therapy or
not trying to do new things

MAKING CONTACT WITH
VULNERABLE/DEPENDENT CHILD
• Ask direct contact with the VC/DC
• Two chair technique
• Imagery
• Empathic confrontation

BYPASSING
THE COPING MODE
• Label the Coping Mode
(protector or overcompensator)
• Explain development in childhood &
empathize with its adaptive value
• Link to trigger events

Bypassing the Coping Mode
• Review pros and cons in the present
(= cognitive technique)
• Empathic confrontation
• Motivate & push for behavioral change
• Two-or-more-chair technique
• Historical role play
• Imagery rescripting

BYPASSING THE COMPLIANT
SURRENDER
(willoos inschikkelijke)
Exercise”
• Review pros and cons of compliant
surrender in the present
• Motivate patient to reduce this
protection
• Short term versus long term
(relationship, job, family, children)
PERFECTIONISTIC
OVERCONTROLER
(denied/
not accessible)
VULNERABLE
CHILD
DEMANDING
PARENT
HEALTHY
ADULT
SELF-
AGGRANDIZER
Obs-Comp PD
HAPPY
CHILD

Obsessive-Compulsive PD
• Get rid of demanding parent mode
• Ask P to reduce Perfectionistic
Overcontroller or Self Aggrandizer:
review pro’s and con’s
• Empathic confrontation
• Explain & push for importance of
emotions, intimacy and social contacts
• Let P experiment with imperfection

BYPASSING
THE COPING MODE
Review pros and cons of perfectionistic
overcontroller present & motivate patient to
reduce this protection

Empathic confrontation
• Expressing understanding about the
patient’s schemas and schema-driven
behaviour while simultaneously confronting
the need for change
• Confront in a friendly, not punitive, way
• Confront in a personal way
• Make connections between behaviour,
schemas and modes and childhood
experiences
• Pay attention to the emotions that might be
triggered

Empathic confrontation: example
overcontroller
• This happens quite often that you interrupt me, to tell me
that I don’t exactly understand you.
• I really understand that you feel that it is necessary that
every fact and every detail is exactly right, and that you
want to be absolutely sure that everything I say is
correct. I understand that your controlling side then gets
active, and wants to take control over our conversation.
• Remember, you developed this side because your father
was extremely critical to you when you made a mistake
or forgot to report every detail.
• Although I understand that this side is afraid that if it
does not control whether what I am thinking and saying
is correct, I really want to ask you to reduce this side and
let me speak, even when not every detail is correct.

• The first reason for this is that I find these
interruptions, to be honost, quite annoying. Your
perfectionistic overcontroller distracts me from what I
am trying to say.
• The second reason is that I feel that letting the
overcontroller control you and me so much is that it
prevents us to have real contact. I feel that it is much
more important to attend to the emotional sides of
your problems, and not to whether every factual detail
is 100% correct. By letting the overcontroller rule our
sessions, I cannot contact little John and address his
needs. And when I cannot do that, the loneliness and
the emotional needs of this side of you cannot be
addressed, and if they cannot be addressed you will
not recover from your problems.
• So that is why I want you to try to stop letting the
overcontroller rule your behaviour, and give both
room to me and to the mode of little John, because
little John and I also have the right to take part in the
conversation.

Obsessive-Compulsive PD
Excersize:
Empathic confrontation of the
overcontroller

DAG 2

Punitive parent:
Guilt inducing parent
• Parent(s) are excessively dependent on
the child
• Separation means danger
• Parent(s) punish autonomy
• FUNCTIONAL DEPENDENCY
• EMOTIONAL DEPENDENCY

COMPLIANT
SURRENDER
DEPENDENT
CHILD
&
ABANDONED/ABUSED
CHILD
PUNITIVE
PARENT
(punishes
Autonomy,
Guilt inducing)
HEALTHY
ADULT
Dependent PD
HAPPY
CHILD

FIGHTING THE GUILT INDUCING
PARENT (PUNITIVE OR DEMANDING)
• Fight the GP, PP or DP:
• Ttwo chair technique therapist combats GP, PP
or DP or dialogue between HA and GP,
• Educate about universal needs and feelings
• Imagery exercise
• Use CBT to develop alternative perspectives on
needs, feelings and normal life problems, like
making a mistake
• Replacement of strict rigid rules by more
adaptive moral standards

Experiential Techniques
• Imagery Rescripting
• Two-or-more-chair Technique
• Role Play

Imagery Rescripting: rationale
• Change the meaning of the original
experiences that contributed to the
development of schemas and modes
• Imagery has stronger emotional and
memory effects than verbal processing
Pathways to childhood
memory
Safe
Place
Present
Problem
Childhood
memory
Instruction Instruction
Instruction
Spontaneous Spontaneous

Imagery Rescripting: rationale
• Identify those schemas that are relevant
for the mode of your patient
• Experience schemas on affective level
• Help patients link on an emotional level
the origins of their schemas in childhood
and adolescence with problems in their
current lives

Important
• Imagery is not the same as exposure
• Stop the image at the right moment
• Imagery and rescripting for traumatic
experiences: not in the beginning of the
therapy

Dependent PD
Excersize:
Imagery rescripting
Guilt inducing parent

Optimale verwerking van correctieve emotionele ervaringen
Window of Tolerance
(Siegel, 1999; Ogden, 2006)
Too much emotion
(hyperarousal)
Overcompensation
Emotionally flooded,
fearfull , angry,
flashbacks, nightmares,
High risk behaviour
Efforts to reduce : abuse of
alcohol and drugs,
automutilation, suïcide attempt
Surrender= freeze
Terrified, frozen, mute
dissociatie.
High arousal coupled
with physical immobility
Optimal arousal Encompassing both high emotion and states of
calm and relaxation in which emotions can be
tolrated and information can be integrated
Little emotion
(hypoarousal)
Flat affect, numb, empty, collapsed
Cognitively dissociated , inabbility to think
Helpless and hopeless
Efforts to reduce : abuse of alcohol and drugs, automutilation,
suïcide attempt

Window of Tolerance
• Influenced by intelligence, working memory capacity,
temperament, stressors, etc.
• Patients can only integrate corrective emotional
experiences when they are within their Window of
Tolerance
• Dysfunctional behaviours are (dysfunctional) attempts
to regulate distress by a person striving to be within
the Window of Tolerance
• Need for process assessment
• Need for a more functional affect regulation

Implications for ST
• Constant assessment of modes
• Constant assessment of needs
• Be aware of re-traumatization: don’t let
patients relive traumatic moments
• Phase experiential exercises
• Work with soothing / bonding / transitional
objects
• Be validating
• Teach patients functional ways of coping
• Have fun

How?
Through the therapeutic
relationship

Activation of schemas of the
therapist
(Counter transference)
© H. van Genderen
93

Schema activation
1. Avoidant behaviour (missing sessions/
arriving too late, doesn’t do homework)
2. Crisis (relapse in depression/ somatic
complaints)
3. Dependent behaviour towards therapist
4. Compliant surrender towards therapist
© H. van Genderen
94

© H. van Genderen
95
DIFFICULT
COMBINATIONS OF
SCHEMAS OR MODES!

© H. van Genderen
96
!
!
COMPLEMENTARITY
Stagnation
Alienation
Abuse
!
!

© H. van Genderen
97
!
SIMILARITY OF SCHEMAS
Stagnation through
identification
Alienation
Conflict

How to deal with schema
activation?
Take care:
Is it caused by the behaviour of the
Patient?
Or is it activation of your own schema?
In case of problems with own schemas:
Seek help (supervision)
© H. van Genderen
98

AVOIDANT
& DETACHED
PROTECTOR
(& COMPLIANT
SURRENDER)
LONELY/INFERIOR
CHILD
&
ABANDONED/ABUSED
CHILD
PUNITIVE
PARENT
HEALTHY
ADULT
Avoidant PD
HAPPY
CHILD

Avoidant PD
• Inept and inferior: low self-esteem
• Emotionally abused or abandoned in
childhood
• NEEDS:
- Nurturance and acceptance
- Freedom to express needs and
emotions

Avoidant PD
Recognize the modes of the
Avoidant PD

Empathic confrontation
• Expressing understanding about the
patient’s schemas and schema-driven
behaviour while simultaneously
confronting the need for change
• Confront in a friendly, not punitive, way
• Confront in a personal way
• Make connections between behaviour,
schema’s and modes and childhood
experiences
• Pay attention to the emotions that might be
triggered

Empathic confrontation:
example Avoidance
• So you have reported ill again when your boss provoked you.
• I really understand that you feel badly treated and that you are
angry at your boss, but that your detached protector side thinks
that it is not wise to express your anger because this was severely
punished when you was a child.
• Although I understand that you are afraid that your boss will
punish you, when you are assertive, just like your father did, I still
want you to discuss the whole thing with your boss and to express
your opinion.
• Because I think this is a healthier way of dealing with these
problems than reporting ill.
• And because I think that you have the fundamental right, just like
everybody else, to express your opinion; it is not okay what you
have been taught when you were a child.
• (You may refer to the fundamental human rights (UN))

Avoidant PD
AVOIDANT & DETACHED PROTECTOR:
• Push to less avoidance of
– Feeling
– Social contacts and roles
– Intimacy
– Making choices
– Having opinions and expressing them
What are the needs of the child?
Two chair technique

Two-chair technique
with the avoidant protector
• State that the avoidant mode is active
• Put this mode in a separate chair and
let this mode express its opinion
• Ask the patient to go back to original
chair
• The Healthy Adult (or the Therapist)
addresses the Dysfunctional Mode
• Express needs of the patient
105

Multiple-chair Technique
When the Dysfunctional Coping Mode and
the Punitive Parent alternate quickly
• Give each Mode a chair
• Discuss with or fight against each mode
• Focus on the reaction of the Child Mode
• Help Child or Healthy Adult to express
needs!
106

Avoidant PD
Excersize:
Two chair technique
AVOIDANT & DETACHED
PROTECTOR:
Pathways to childhood
memory
Safe
Place
Present
Problem
Childhood
memory
Instruction Instruction
Instruction
Spontaneous Spontaneous

Avoidant PD
Excersize:
Imagery rescripting
PUNITIVE PARENT MODE

DAG 3
PERFECTIONISTIC
OVERCONTROLER
(denied/
not accessible)
VULNERABLE
CHILD
DEMANDING
PARENT
HEALTHY
ADULT
SELF-
AGGRANDIZER
Obs-Comp PD
HAPPY
CHILD

Obsessive-compulsive PD
Exercise:
Imagery rescripting
Demanding parent

TREATMENT OBJECTIVES:
healthy adult mode
• Help patient to strengthen the
Healthy Adult Mode
• Therapist / therapeutic
relationship is model

Healthy Choices
• Aim = to improve mental health
• Motivation: explain that choices so far
were based on dysfunctional modes
(name them)
• Help patient to reflect on what (s)he really
wants
• Support with making healthy choices and
the fears that they raise
• Ask next session how it went!

Strenghtening The Healthy Adult
• Behavioural techniques
• Two chair technique
• Imagery rescripting
• Teach healthy attitudes
• Push towards healthy choices:
– Education / work
– Hobbies
– Friends
– Partner:
Breaking through dysfunctional partner choices;
Learning to make a healthy partner choice

Empathic confrontation to
push for behavioural change
• Aim = motivate & push for behavioural
change
• Step 1: Empathise with the function of the
original dysfunctional behaviour & link with
schema mode
• Step 2: Nevertheless, ask for behavioural
change
• Step 3: Motivate this

Happy Child
Happy, Spontaneous Joyful
• Make fun during sessions
• Stimulate play outside sessions

Happy Child
Demonstration:
Pushing for spontaneity
COMPLIANT
SURRENDER
DEPENDENT
CHILD
&
ABANDONED/ABUSED
CHILD
PUNITIVE
PARENT
(punishes
Autonomy,
Guilt inducing)
HEALTHY
ADULT
Dependent PD
HAPPY
CHILD

Experiential Techniques
• Two-or-more-chair Technique
• Historical role Play
• Imagery Rescripting

Historical Role Play
• Find relevant events in the past
• P. gets more insight in her own part in
the interaction
• P. gets more insight in the motivation her
parents could have had
• Changing interpretation of the situation
• Therapist can give feedback after
playing the child role
• Try out new behaviour from a healthy
perspective
© H. van Genderen
121

Aim is NOT
• That patient feels guilty of having done it wrong
- But patient gets new insight (in own part, in possible
perspective of the parents)
- and change of the interpretation of the original situation
• Another perspective, does not “excuse” the parents
for not meeting the needs of the child
• Behavioral rehearsal
- But changes in emotions and cognitions
• Immediate change in present behavior
- Don’t expect that!
• In sum: aim is change on schema level

Historical Role Play: Preparation
Discuss a behavioral pattern that gets
stuck every time
P. thinks of a relevant event in the past
which is similar to patterns in the present
© H. van Genderen
123
© H. van Genderen
32
Historical role play
1.
P. = Child
T. = the other person
Original situation
Conclusion about myself:
Assumed perspective of the other person:
2.
P.= the other person
T.= Child
Original situation: role switching
P. Experiences the perspective of the other
Alternative conclusion about myself:
Alternative assumed perspective of the other person:
3.
P. = Child
T. = the other person
P. Now tries out a new behavior
Alternative conclusion about myself:
Alternative assumed perspective of the other person:
Original conclusion about myself:
Implications for the future:

Avoidant PD
Exercise:
Historical role play
Punitive parent and autonomy

Protocol sessions 26-40
• Start asking about:
– Audiotape & last week; focus more on
behavioural change
• Detect which mode is (was) active
• Focus more on present life
– How to address current problems
– Push towards behavioural change
– Support this with schema-mode
techniques and flashcards

Protocol sessions 26-40
• Also focus on therapeutic relationship
– Discuss dysfunctional schema mode
in the relationship
– Help to achieve healthy view
– Push healthy behaviour in the
therapeutic relationship

Protocol sessions 41-50
(booster sessions)
• Focus on last month
Especially behavioural changes
• Detect what modes are / were active
• Praise healthy attitudes and behaviours
• View problems as challenges
Don’t criticize or catastrophize ‘relapse
Formulate problems as choices
• Educate:
old modes don’t disappear completely, but will
have less influence if you practice healthy ways
• Motivate to healthy choices and autonomy

Empathic confrontation to
push for behavioural change
Aim = motivate & push for behavioural
change
• Step 1: empathise with the function of the
original dysfunctional behaviour & link
with schema mode
• Step 2: nevertheless, ask for behavioural
change
• Step 3: motivate this

Behavioural change
• Aim = behavioural change
• Motivation: explain that new behaviour is
necessary to come to a final change
• Rehearse in role plays or using imagery;
give (informal) model and ask patient to try
out
• Ask next session how it went!

Learning to express anger
• Being afraid of feeling and expressing
irritation and anger is important in
Cluster-C
• Patients need to learn that it is normal
and healthy to express anger and be
assertive

Learning to express anger
• Practice by:
– Role plays
– Imagery exercises
– Writing assignments (e.g. write letter
expressing anger; don t send)
– Expressing anger towards T.
– Drama Therapy
– Playful exercizes like tug-of-war

Cluster C PD
Exercise:
Expressing Anger

DAG 4

Imagery Rescripting: rationale
• Identify those schemas that are relevant
for the mode of your patient
• Experience schemas on affective level
• Help patients link on an emotional level
the origins of their schemas in childhood
and adolescence with problems in their
current lives

Imagery Rescripting:
Patient rescripts
1. Original situation (P. is Child)
2. P. is Healthy Adult who helps the Child
3. P. is Child again: Now he experiences
the support of his own Healthy Adult
T. Paraphrases what H. A. of P. does.

Cluster C PD
Exercise:
Imagery rescripting
Patient rescripts

Autonomy
• Being afraid of feeling and expressing
irritation and anger is important in
Cluster-C
• Patients need to learn that it is normal
and healthy to express anger and be
assertive

Avoidant PD
Exercise:
Pushing for more autonomy

Extra Slides

Coping vragenlijst
Overcompensa,e-
Ik kan erg kritisch zijn over wat anderen
doen of laten.
Ik fantaseer over beroemd, rijk, belangrijk of
succesvol te zijn.
Wanneer ik kritiek krijg, schiet ik meteen in
de verdediging..
Ik heb de neiging anderen te overheersen en
te controleren.

Coping vragenlijst
Overgave--
Bij problemen of moeilijkheden denk ik: “Zie je
wel, dit overkomt mij weer”.
Als er moeilijkheden zijn, ben ik geneigd om bij
de pakken neer te gaan zitten.
Als anderen mij slecht behandelen, laat ik dat
gebeuren.
Ik laat mijn leven door anderen bepalen.

Coping vragenlijst
Vermijding-
-
Ik ga liever geen intieme vriendschappen of
relaties aan.
Ik ga confrontaties liefst uit de weg.
Het is beter om je gevoel zoveel mogelijk uit te
schakelen
Ik houd het graag oppervlakkig.
