BY ORDER OF THE
SECRETARY OF THE AIR FORCE
AIR FORCE INSTRUCTION 48-127
26 FEBRUARY 2016
Aerospace Medicine
OCCUPATIONAL NOISE AND
HEARING CONSERVATION PROGRAM
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
ACCESSIBILITY: Publications and forms are available for downloading or ordering on the
e-Publishing website at www.e-publishing.af.mil/
RELEASABILITY: There are no releasability restrictions on this publication.
OPR: HQ AF/SG3/P
Supersedes: AFOSHSTD48-20,
10 May 2013
Certified by: HQ AF/SG3/5
(Maj Gen Roosevelt Allen, Jr)
Pages: 62
This Air Force Instruction (AFI) implements Air Force Policy Directive (AFPD) 48-1,
Aerospace Medicine Enterprise; Occupational Safety and Health Administration (OSHA) Title
29, Code of Federal Regulations (CFR), 1910.95, Occupational Noise Exposure; Title 5, CFR,
Volume 1, Part 339, Medical Qualification Determinations; and DoDI 6055.12, Hearing
Conservation Program, except for military unique situations. This instruction administers the
Air Force (AF) Hearing Conservation Program (HCP) to prevent occupational illness and
injuries under Federal and Department of Defense (DoD) references. This instruction requires
collecting and maintaining information protected by the Privacy Act (PA) of 1974. The
authorities to collect and maintain the records prescribed in this publication are Title 10 United
States Code (USC) Chapter 55, Medical and Dental Care, 10 USC § 8013, Power and Duties of
the Secretary of the Air Force, and Executive Order 9397. Forms affected by the PA have an
appropriate PA statement. The applicable PA System of Records Notices (SORN) Defense
Health Agency (DHA) 07, Military Health Information System, DHA 19, DoD Occupational
Environmental Health Readiness System-Industrial Hygiene, and F044 F SG E, Electronic
Medical Records System apply. Ensure that all records created as a result of processes
prescribed in this publication are maintained IAW Air Force Manual (AFMAN) 33-363,
Management of Records, and disposed of IAW the Air Force Records Disposition Schedule
(RDS) in the Air Force Records Information Management System (AFRIMS). This AFI may be
supplemented at any level, but all supplements that directly implement this publication must be
routed to Air Force Medical Support Agency/Public Health and Preventive Medicine Branch
(AFMSA/SG3PM) for coordination prior to certification and approval. Refer recommended
changes and questions to the Office of Primary Responsibility (OPR) using the AF Form 847,

2 AFI48-127 26 FEBRUARY 2016
Recommendation for Change of Publication; route AF Forms 847 from the field through the
appropriate functional chain of command. The authorities to waive wing/unit level requirements
in this publication are identified with a Tier number (“T-0, T-1, T-2, T-3”) following the
compliance statement. See AFI 33-360, Publications and Forms Management, Table 1.1. for a
description of the authorities associated with the Tier numbers. Submit requests for waivers
through the chain of command to the appropriate Tier waiver approval authority, or alternatively,
to the publication OPR for non-tiered compliance items. The use of the name or mark of any
specific manufacturer, commercial product, commodity, or service in this publication does not
imply endorsement by the Air Force.
All AF Active Duty, Reserve, and National Guard military and civilian personnel (including
Reserve technicians and Reserve Component military Reserve technicians) are covered by this
instruction. (Note: Air Reserve (AR) and Air National Guard (ANG) will collectively be
referred to as Air Reserve Component (ARC)). This includes all appropriated fund, non-
appropriated fund, seasonal, and temporary personnel. Foreign nationals employed by the
United States Air Force (USAF) under a direct or indirect hire arrangement are also included
unless exempt by other agreements. Foreign national military personnel assigned to the USAF
are included, unless other preventive measures and medical care are not provided by AF.
Contractors must comply with state and federal noise standards, and are exempt from compliance
with this instruction. Contract personnel should not be enrolled in the AF HCP unless HCP
services are included in the contract. HCP services are not normally included in contracts. This
instruction does not apply to community noise situations. Referenced American National
Standards Institute’s (ANSI) standards may be obtained for a fee from ANSI at
http://webstore.ansi.org.
SUMMARY OF CHANGES
This document, AFI 48-127, replaces Air Force Occupational Safety and Health (AFOSH)
Standard 48-20, Occupational Noise and Hearing Conservation Program, has been substantially
revised and must be completely reviewed. This instruction identifies the Tier waiver authorities
as approved by the Inspector General Advisory Board. Major changes include baseline
audiograms for all new officer and enlisted accessions and hearing related fitness and risk
evaluations are to close 45 days after determination that an evaluation is required.
1. Overview. ................................................................................................................ 3
2. Roles and Responsibilities. ..................................................................................... 4
AFI48-127 26 FEBRUARY 2016 3
Attachment 1— GLOSSARY OF REFERENCES AND SUPPORTING INFORMATION 27
Attachment 2— HAZARDOUS NOISE SURVEILLANCE 36
Attachment 3— CERTIFICATION AND EQUIPMENT STANDARDS 46
Attachment 4— HEARING PROTECTION 49
Attachment 5— FITNESS AND RISK EVALUATIONS 56
Attachment 6— HEARING CONSERVATION DIAGNOSTIC CENTERS
(HCDC)/HEARING CONSERVATION CENTERS (HCC) AND
REFERRAL CRITERIA 59
Attachment 7— OWCP HEARING LOSS MEDICAL REQUIREMENTS AS
PARAPHRASED FROM DOL OWCP HEARING LOSS SECTION
INSTRUCTIONS 62
1. Overview.
1.1. The USAF HCP is a component of the Occupational and Environmental Health (OEH)
Program, and is a command-driven program designed to reduce or eliminate hazardous noise
exposure to workers and protect workers from the harmful effects of hazardous noise, while
enhancing combat and operational capabilities. This process must occur across the full life
cycle of acquisition, sustainment, and support for weapons systems, munitions and other
materiel systems. This requires identifying all areas where workers are exposed to hazardous
noise and reducing exposure through engineering or administrative controls, or personal
protective equipment (PPE). (Also, refer to AFI 91-203, Air Force Consolidated
Occupational Safety Instruction). One key to accomplishing these goals is an education
program that explains the individual’s role in protecting their hearing to include hazardous
noise exposures on and off duty and how to mitigate those threats.
1.2. DoDI 6055.12 requires all DoD Components to implement a comprehensive program
and written plan for hearing conservation when personnel are occupationally exposed as
described in DoDI 6055.12. This instruction meets the intent and requirements of DoDI
6055.12 and reflects the unique functions, capabilities, and procedures of the Air Force HCP.
1.3. For Joint Bases, this instruction is followed unless specific processes and provisions,
meeting the intent and requirements of OSHA and DoDI 6055.12, are detailed in the
Memorandum of Agreement.
1.4. IAW AFI 48-145, Occupational and Environmental Health Program, hearing
conservation issues will be considered through the Occupational and Environmental Health
Working Group (OEHWG) just as any other occupational exposure.
1.5. HCP requirements should be covered with other OEH program responsibilities in
memorandums of agreement as discussed in AFI 48-145.
1.6. This AFI does not encompass audiograms for new accessions (officer and enlisted),
conducted by the Department of Defense Hearing Center of Excellence.
4 AFI48-127 26 FEBRUARY 2016
2. Roles and Responsibilities.
2.1. Deputy Assistant Secretary of the Air Force for Environment, Safety and
Infrastructure(SAF/IEE) will:
2.1.1. As delegated by the Assistant Secretary of the Air Force for Installations,
Environment and Energy (SAF/IE), provide policy, guidance, direction and oversight of
all matters pertaining to the formulation, review and execution of plans, policies,
programs and budgets relative to the Environment, Safety and Occupational Health
(ESOH) programs. Oversee implementation of those programs IAW AFPD 90-8,
Environment, Safety and Occupational Health Management and Risk Management.
2.1.2. Ensure Air Force operations involving occupational and combat-related exposure
to hazardous noise establish and maintain HCPs in compliance with Federal and DoD
requirements. Such programs encompass the minimum requirements in DoDI 6055.12.
2.2. Air Force Surgeon General (AF/SG) will:
2.2.1. Provide strategic direction and policy to execute the AF HCP.
2.2.2. Appoint the AF/SG’s Audiology Consultant.
2.2.3. Support Combatant Commanders to establish hearing testing capabilities in
theaters of operation whenever appropriate.
2.3. Surgeon General Aerospace Medicine Policy and Operations Division (AF/SG3P) will:
2.3.1. Serve as the principal AF point of contact with Federal and DoD agencies
regulating occupational exposure to hazardous noise.
2.3.2. Develop policy and provide coordination on hearing conservation matters in the
AF.
2.3.3. Provide policy execution guidance to support installations in interpreting and
implementing the HCP requirements in DoDI 6055.12 and this instruction.
2.3.4. In conjunction with the AF SG’s Audiology Consultant, identify USAF Hearing
Conservation Diagnostic Centers (HCDC) and Hearing Conservation Centers (HCC)
used for the evaluation of personnel with hearing loss in support of the HCP. Reference
Attachment 6 for a list of authorized HCDC/HCCs.
2.4. Headquarters Air Force Safety Center (AFSEC) will coordinate with AF/SG3P for
safety requirements associated with hazardous noise exposure (T-0).
2.5. Air Force Medical Operations Agency (AFMOA) will:
2.5.1. Allocate funding to resource and equip installations to assist with meeting the
HCP requirements (T-1).
2.5.2. Ensure the gaining Military Treatment Facilities (MTFs) have funds to send all
new Air Force audiologists to a hearing conservation program-training course at USAF
School of Aerospace Medicine (USAFSAM) within one year of assignment to first duty
station for active duty or within the first year of employment for civilian audiologists.
Contract audiologists hired to perform hearing conservation program duties may attend
AFI48-127 26 FEBRUARY 2016 5
training at USAFSAM or a civilian equivalent training approved by the AF SG’s
Audiology Consultant in accordance with contract management policy (T-0).
2.6. Major Commands (MAJCOMs) will:
2.6.1. Coordinate with the AF/SG’s audiology consultant to identify and designate a
hearing conservation consultant (e.g., a regional HCDC/HCC or an Occupational
Medicine clinic) to oversee the command HCP.
2.6.2. Allocate resources to staff and equip the HCDC/HCCs within their area of
responsibility to provide regional HC referral support. Reference Attachment 6 for
additional information.
2.6.2.1. HCDCs and HCCs must consist of an audiologist and support staff.
2.6.2.2. At a minimum, testing capabilities will include diagnostic audiometer
equipment sufficient to complete a full comprehensive hearing exam, a full range of
immittance, electrophysiological, and otoacoustic emissions equipment.
2.6.3. Utilize the ESOH Council as the executive forum to oversee the performance of
the HCP and advocate for resource requirements when necessary.
2.7. Within Air Education and Training Command:
2.7.1. The 2nd AF will ensure all basic military trainees will receive an audiogram prior
to or within the first week of training.
2.7.2. The Air University Commander will ensure all Basic Officer Training, Academy
of Military Science and direct Commissioned Officer Training students will receive an
audiogram during training.
2.8. Assistant Secretary of the Air Force for Acquisition (SAF/AQ) will:
2.8.1. Ensure Acquisitions Program Offices include personnel noise study data on
systems in the Programmatic Environment, Safety, and Occupational Health Evaluations
(PESHE) and obtain formal coordination of new and updated PESHEs from their
supporting Surgeon General offices, as required by AFI 63-101/20-101, Integrated
Lifecycle Management. The coordinating Surgeon General office shall provide copies of
the PESHE to the USAFSAM Occupational and Environmental Health Department
(USAFSAM/OE).
2.8.2. Ensure new equipment and weapons systems being considered for fielding have
the lowest sound emission levels that are technologically and economically possible, and
compatible with performance and environmental requirements. Title 42 USC Section
4914, Development of Low-Noise-Emission Products, applies.
2.9. Commander, Air Force Materiel Command (AFMC) will ensure that the AF Research
Laboratory (AFRL) 711th Human Performance Wing (HPW) will:
2.9.1. Appoint an occupational medicine consultant who provides consultation for the
AF HCP (T-2).
2.9.2. Execute the research and consultative missions related to noise evaluation and
control via Acoustic and Vibration Center of Excellence (T-2). The Acoustic and
Vibration Center of Excellence will have standing members including the 711

6 AFI48-127 26 FEBRUARY 2016
HPW/Human Effectiveness Directorate (RH), USAFSAM/OE, and USAFSAM Public
Health (USAFSAM/PH) (T-2). The Acoustic and Vibration Center of Excellence single
point of contact (POC) is the ESOH Service Center at [email protected],
888-232-3764, or DSN798-3764. Direct all requests for support and any questions about
these responsibilities to this POC. The Acoustic and Vibration Center of Excellence
will:
2.9.2.1. Provide consultative services to measure, evaluate, and recommend controls
and solutions for occupational noise concerns within the AF (T-2). Develop and
recommend noise criteria, assessment, and control strategies to acquisition programs
(T-2).
2.9.2.2. Conduct research relative to noise exposure criteria and speech intelligibility
(T-2).
2.9.2.3. Represent the USAF on ANSI accredited standards committees relative to
noise S1 (acoustics), S3 (bioacoustics), and S12 (noise) (T-2).
2.9.2.4. Conduct acoustic research relative to human performance in USAF
environments (T-2).
2.9.2.5. Conduct measurements to quantify the performance of attenuation of hearing
protectors, and attenuation and speech intelligibility of communication
headsets/microphones (T-2).
2.9.2.6. Characterize the ground run-up, flyover, and interior noise levels of aircraft
(T-2).
2.9.2.7. Characterize high-level continuous noise, greater than 130 decibels (dB), and
impulsive noise greater than 170 dB (T-2).
2.9.2.8. Recommend to AF/SG, USAF exposure criteria for continuous and
impulsive noise (T-2).
2.9.2.9. Provide data/information and consultation related to historic acoustical
assessments performed by the 711 HPW and professional organizations to base
Bioenvironmental Engineering (BE) (T-2).
2.9.2.10. Provide consultation and assistance on the selection of hearing protectors
(T-2).
2.9.2.11. Provide data/information and consultation on unique or complex acoustic
environments (T-2).
2.9.2.12. Develop guidance on hierarchy of noise measurement techniques (T-2).
2.9.2.13. Represent USAF with federal agencies and national professional
organizations that set standards and standards of practice in the ESOH disciplines (T-
2).
2.9.2.14. Maintain a repository of relevant references in noise and hearing protection
(T-2).
2.9.2.15. Develop and provide guidance and oversight for the AF HCP (T-2).
AFI48-127 26 FEBRUARY 2016 7
2.9.2.16. Evaluate AF HCP effectiveness based performance measures as defined by
AFMSA, HAF, and DoDI 6055.12 (T-0). At a minimum, performance measures
include the incidence of significant threshold shift (STS) and permanent threshold
shift (PTS), and audiogram compliance rates for all workers enrolled in the HCP
program (including threshold shift follow-up rates).
2.9.2.17. Provide AFMSA/SG3PM, MAJCOMs and base-specific reports
communicating the results of the performance measures on a routine basis or at least
annually (T-2).
2.9.2.18. Evaluate and report recommendations for corrective action to installation
level Hearing Conservation Program Manager (HCPM) and to the MAJCOMs
(SGPM) to improve data quality in the Department of Defense Occupational and
Environmental Health Readiness System (DOEHRS) Data Repository (DR) on a
routine basis (at least annually) and upon request (T-2).
2.9.2.19. Appoint an appropriately trained audiologist to serve as the AF Hearing
Conservation Program Manager (AF HCPM). This individual will serve as a primary
representative to the DoD HC and Readiness working group, the DoD DOEHRS-HC
functional users group and as the consultant for DOEHRS-HC and DR in the Air
Force (T-1).
2.9.2.20. Provide training to support the HCP (T-2).
2.9.2.20.1. Provide DR orientation and program management training for newly
assigned military, civilian and contract AF audiologists, as needed (T-2).
2.9.2.20.2. Conduct formal Council for Accreditation in Occupational Hearing
Conservation (CAOHC)-approved training for DoD personnel (military and
civilian) who perform audiograms (T-2). Reference Attachment 3.
2.9.2.20.2.1. Provide AF certification numbers to students upon completion
of CAOHC training (T-2). If AF certification numbers are unavailable the last
day of training, they will be provided within 10 days of CAOHC training.
2.9.2.20.2.2. Track HC certification numbers for personnel who are trained
IAW the CAOHC (T-2). Note: AF personnel who receive CAOHC-approved
training at civilian agencies must register certification information with the
AF HCPM and receive an AF certification number prior to conducting
audiometric testing. AF personnel who are CAOHC trained by a DoD
component will use the certification number issued by that Service.
2.9.2.20.3. Conduct training for Public Health (PH) Officers and skill-level
appropriate 4E0X1 using course material that addresses components of HCP
administration/management (T-2). Provide CAOHC hands-on and didactic
DOEHRS-HC training for 4E0X1 personnel for the HCP (T-2).
2.9.2.20.4. Conduct training for providers on audiogram review, audiogram
consultation, referrals, and fitness and risk evaluations (T-2).
2.9.2.20.5. Conduct training for BE technicians and officers that addresses
identification, assessment, control and documentation (in DOEHRS-Industrial
Hygiene (IH)) of hazardous noise exposures as outlined by Federal, DoD and AF
8 AFI48-127 26 FEBRUARY 2016
standards (T-2).
2.9.2.20.6. Provide HC orientation training for newly assigned military, civilian,
and contract AF audiologists, as needed (T-2).
2.9.2.20.7. Produce annual reports on the percentage of hazardous noise
workplaces characterized and the index of unacceptable noise exposures, as
outlined in DoDI 6055.12, and provide to AFMSA/SG3PB (T-0).
2.10. Wing Commanders will:
2.10.1. Provide oversight and support for an installation hazardous noise reduction and
protection program (T-1).
2.10.2. Ensure HCP is a standing agenda item for the ESOH Council as outlined in AFI
90-801, Environment, Safety, and Occupational Health Council (T-2). Program
effectiveness will be evaluated; information to be briefed may include the program
performance metrics, as outlined in DoDI 6055.12, the number of shops and personnel on
the program, incidence rate of STS and PTS, percent of workers requiring follow-up, etc.
2.11. Squadron Commanders will:
2.11.1. Ensure workplaces and Workplace Supervisors comply with all AF HCP, DoD,
and OSHA requirements (e.g., workplace noise hazard assessments, ensuring monitoring
of hazardous noise-exposed personnel including pre-placement, periodic, and termination
audiograms; training of noise-exposed personnel, and supplying hearing protection
devices and enforcing use, as appropriate) (T-0).
2.11.2. Participate in the review of the workplace hazards as process owners to identify
actions taken to mitigate hazardous noise (i.e., efforts to procure equipment which does
not generate hazardous noise, applying engineering and administrative controls) (T-2).
2.11.3. Resource engineering controls as the primary means of eliminating exposure to
potentially hazardous noise when feasible (T-0). Apply engineering controls to "military-
unique workplaces", within the constraints of maintaining combat readiness.
2.11.3.1. Assign priorities for noise control resources based on the applicable Risk
Assessment Codes (RAC) IAW DoDI 6055.12 and DoDI 6055.05 (T-0).
2.12. Workplace Supervisors will:
2.12.1. Ensure personnel comply with all AF HCP, DoD, and OSHA requirements (e.g.,
comply with workplace noise hazard assessments, pre-placement, periodic, and
termination audiograms, training, and use of hearing protection devices as appropriate)
(T-0).
2.12.2. Use Bioenvironmental Engineering (BE) recommendations for engineering
controls as the primary means of eliminating exposure to potentially hazardous noise and
protecting the hearing of assigned personnel to ensure an individual’s daily noise dose
does not exceed an 8-hour time weighted average (TWA) of 85 decibels A-weighted
(dBA) (T-0). Limiting exposure time, increasing distance from noise sources (in some
cases), and ensuring all workers are correctly using approved (Certified Protective
Equipment List) hearing protection are secondary means of limiting the hazardous noise
dose when engineering controls are not feasible to control hazardous noise.
AFI48-127 26 FEBRUARY 2016 9
2.12.2.1. Explore and use all practical design approaches as recommended by BE to
reduce noise levels to below hazardous levels (T-0).
2.12.3. Mark “hazardous noise areas” and “equipment” (as identified by BE) with signs
and/or decals (T-0). As a minimum, all signs and decals will comply with DoDI 6055.12.
Signs and/or decals will describe (in words or with other visual symbols) the potential
hazard and the required protective measures (e.g., “Caution”, “Hazardous Noise”,
“Hearing Protection Required When in Operation”). For potentially hazardous noise
areas, signs will be located at their entrances or boundaries, including pathways leading
to hazardous noise areas. Reference Attachment 2.1.3for more information.
2.12.3.1. Maintain a supply of approved hearing protection devices (HPDs) along
pathways leading to hazardous noise areas or equipment (T-0).
2.12.3.2. Ensure personnel carry hearing protectors with them when working in or
entering designated "hazardous noise areas" and wear their hearing protection devices
when noise sources are operating, regardless of exposure time. (T-0). This includes
visitors, temporary or transient personnel (i.e., repair technicians), aircrew, and
ground based controllers entering hazardous noise areas.
2.12.3.3. In consultation with BE, ensure each tool or piece of equipment producing
noise levels greater than or equal to 85 dBA, including vehicles, is clearly marked to
alert personnel of the potential hazard (T-0). Exception: When an entire space is
designated a "hazardous noise area," and the equipment is stationary. In addition,
exteriors of military combatant equipment are excluded from this requirement.
2.12.4. Notify BE/PH personnel within 3 calendar days for a follow-up BE noise level
survey if workplace equipment, or practices and procedures involving potentially
hazardous noise change (T-2). Assure that no hazardous noise producing equipment is
operated beyond an initial 30 day implementation period unless it has been assessed by
BE and all required controls have been implemented.(T-2).
2.12.5. Ensure new equipment being considered for purchase has the lowest sound
emission levels that are technologically and economically possible and compatible with
performance and environmental requirements (T-0). Title 42 USC Section 4914 applies.
2.12.6. Consult BEs on appropriate acoustics in specifications for all new facilities,
equipment, and substantial modification projects (T-0). The objective is to ensure, if
possible, a steady-state level less than 85 dBA at all personnel locations during normal
operations.
2.12.7. Ensure compliance and availability of approved HPDs for workers exposed to
hazardous noise (T-0).
2.12.7.1. Only purchase earmuffs, disposable plugs, and/or other hearing protection
approved by BE (T-1). If approved hearing protection is no longer available, consult
with BE for suitable replacement (T-1).
2.12.7.2. Consult with BE, PH, and the Occupational Medicine consultant before
purchasing custom molded earplugs for the unit (T-1). Reference Attachment 4 for
more information.
10 AFI48-127 26 FEBRUARY 2016
2.12.8. Instruct personnel on the HCP, the care/hygiene of their HPDs, and ensure their
HPDs are properly maintained (T-0). Reference Attachment 4 for more information.
2.12.9. Ensure workers with an occupational exposure to hazardous noise complete an
initial/reference audiogram and receive HCP training from PH prior to but not to exceed
30 days before the date of the workers’ initial exposure to hazardous noise (T-0).
2.12.10. Conduct initial and annual workplace-specific hearing conservation training on
shop or unit hazardous noise exposures and equipment for all personnel exposed to
hazardous noise regardless of whether or not they are on the AF HCP (T-0). Consult PH
for training materials (T-1).
2.12.10.1. Document all training on the worker’s AF Form 55, Record of Training, or
equivalent (T-2).
2.12.10.2. IAW with OSHA, training must cover:
2.12.10.2.1. The effects of noise on hearing, on and off duty sources of hazardous
noise, the purpose of hearing protection, and the proper use of hearing protection
devices (T-0). Recommend the need to wear hearing protection off duty when
exposed to hazardous noise (T-0).
2.12.10.2.2. The advantages, disadvantages, and attenuation of various types of
hearing protectors (T-0).
2.12.10.2.3. Instructions on use, proper wear, and care of hearing protectors (T-
0).
2.12.10.2.4. Counsel on the interaction between HPDs interfacing with other
forms of PPE (T-1). Some types of PPE, such as eyewear, can create ill-fitting
circumaural HPDs if fit of all PPE is not evaluated collectively. Reference
Attachment 4 for details.
2.12.10.2.5. The purpose of audiometric testing (T-0).
2.12.10.2.6. Hearing loss and how it may lead to disqualification from current
duties if hearing is critical to job performance (T-1).
2.12.10.2.7. Mandatory requirement of assigned protective equipment, and the
administrative actions that may follow for failure to wear (T-0).
2.12.11. Ensure personnel on the HCP are made available for examination and attend
scheduled medical appointments (T-1). All reference hearing tests and the two noise-free
follow-up tests after a positive STS will be preceded by at least 14 hours without
exposure to hazardous noise. This requirement will not be met by wearing hearing
protective devices (T-0).
2.12.12. Inform BE/PH personnel of each new operation, job, or process before it is
implemented (T-2).
2.12.13. Ensure all hazardous noise areas above the dual hearing protection requirement
are evaluated for a RAC to assist commanders in tracking corrective actions and
mitigating the source (T-0).
AFI48-127 26 FEBRUARY 2016 11
2.12.14. Recommend the use of HPDs and other noise control methods outside the
workplace, including the use of HPDs for installation recreation facilities with hazardous
noise sources (auto hobby, skeet, etc.) (T-0).
2.12.15. Provide a copy of 29 CFR 1910.95 in the workplace so it is available to
employees (T-0).
2.12.16. Assist with completion of AF Form 1754, Job Capability and Safety Analysis
(T-2). Reference Attachment 5 for details.
2.12.17. IAW OSHA regulation 29 CFR 1910.95 (e), notify each employee exposed at or
above an 8-hour TWA of 85 dBA of the results of the noise monitoring performed by BE
(T-0).
2.12.18. Notify each worker of hazardous noise sources in the workplace as identified by
BE (T-0).
2.12.19. Provide information to BE about work practices and procedures involving
potential exposure to hazardous noise to allow proper surveys and evaluations of the
workplace (T-1).
2.12.20. Update and maintain current rosters of personnel occupationally exposed to
hazardous noise using the Occupational Health Supervisor Module in Aeromedical
Services Information Management System (ASIMS) (T-2). Update rosters at a minimum
of every 6 months (T-2). Ensure that all newly assigned and departing personnel receive
all required audiograms (i.e., pre-placement and termination) in the scheduled timeframe
(T-0).
2.13. Employees with Hazardous Noise Exposure will:
2.13.1. Comply with all hazardous noise control measures whether at work or at
deployed location to reduce exposure to hazardous noise IAW DoDI 6055.12 (T-0).
Employees will:
2.13.1.1. Reduce exposure by properly using hearing protectors and advise others in
the workplace to wear HPD when exposed to hazardous noise IAW OSHA CFR
1910.95 (T-0). Employees are highly encouraged to wear HPDs off duty when
operating hazardous noise producing equipment or tools, including firearms.
2.13.1.1.1. Personnel working in or entering designated "hazardous noise areas"
will always carry hearing protectors with them IAW DoDI 6055.12 (T-0). This
includes visitors, temporary or transient personnel (i.e., repair technicians),
aircrew, and ground based controllers entering hazardous noise areas.
2.13.1.1.2. When noise sources are operating, personnel will wear their HPDs
regardless of exposure time IAW DoDI 6055.12 (T-0).
2.13.1.1.3. Personnel will wear hearing protectors as directed when exposed to
gunfire or artillery fire in test or training situations (T-0).
2.13.2. Maintain HPDs appropriately as instructed by supervisor (reference 2.12.8.) (T-
0).
12 AFI48-127 26 FEBRUARY 2016
2.13.3. Notify supervisor when HPDs no longer appear functional or usable so the HPDs
can be replaced (T-0).
2.13.4. Receive all required audiometric evaluations IAW OSHA 29 CFR 1910.95 and
DoDI 6055.12 (T-0).
2.13.4.1. Personnel will report for appointments to receive required periodic medical
surveillance examination (MSE) (T-0).
2.13.4.2. Personnel will take the HPDs used to the appointment, including any PPE
that is worn in conjunction with HPDs, such as eyewear, that could affect the fit of
HPDs (T-1). Proper fitting technique will be demonstrated at the time of the
audiogram.
2.13.4.3. Employees should not continue to perform duties in hazardous noise if the
examination requirement is not met (T-1).
2.13.5. Report to supervisor or medical personnel conditions that place themselves or
others at risk for accident because of communication difficulty or the inability to hear
warning signals (T-1).
2.13.6. Report to the supervisor any new or changes in operating procedures that affect
workplace hazardous noise exposure and participate in noise exposure surveys and
evaluations by wearing monitoring equipment as requested by BE (T-1).
2.13.7. Identify initiatives and inform supervisors/leadership of opportunities to reduce
or eliminate hazardous noise in their work centers (T-2).
2.14. Directors of Base Personnel (Military and Civilian) will:
2.14.1. Evaluate and reassign personnel, based on medical recommendations, to a
suitable workplace (T-2). Include those awaiting reasonable accommodations in, denied
placement in, or removed from, hazardous noise-related jobs.
2.14.2. Ensure civilian workers receive a pre-placement hearing test/medical clearance
before being hired or transferred into a position that includes duties in a hazardous noise
environment (T-0).
2.14.3. Upon request from the installation level HCPM or the provider, prepare an AF
Form 1754, Part 2, with essential tasks that a worker must perform, at a minimum, to
qualify for or to retain a position to allow the provider to conduct a worker’s fitness and
risk evaluation (T-2).
2.14.4. Report the number of civilian claims filed for noise-induced hearing loss and the
cost of the award to the ESOH Council (T-2).
2.14.5. Ensure Civilian Personnel Office provides the OEHWG and installation level
HCPM information related to any hazardous noise illness or injury claims (T-2).
2.15. Host Installation and/or Organizational Safety Staff will:
2.15.1. Complete the safety analysis called for in this instruction using the AF Form
1754, Part 4, with assistance from shop supervisor. (T-2). Reference Attachment 5 for
details.
AFI48-127 26 FEBRUARY 2016 13
2.15.2. Report noncompliance with the HCP to the supervisor and BE office (T-1).
2.15.3. Identify newly added hazardous noise work tasks or areas noted during periodic
safety inspections to BE (T-2).
2.16. MTF/CC (RMU/GMU/CC for ARC) will:
2.16.1. Ensure a comprehensive HCP is available and appropriately resourced to meet
requirements (T-1).
2.16.2. Provide guidance for successful execution of the HCP at their installation (T-1).
2.16.3. Appoint the audiologist, occupational medicine provider or an experienced flight
surgeon to be the installation level HCPM (T-1). For DOEHRS-HC/DR records
management, a certified 7-level hearing conservationist can assume the HCPM access
level role in the DOEHRS-HC software and on the Data Repository.
2.17. MTF/SGP or ARC/SGP will provide programmatic oversight of the HCP program and
coordinate all Aerospace Medicine activities related to HCP (T-1).
2.18. The Squadron/CC or ARC/SGP under whose command the HCP resides will:
2.18.1. Ensure HCP personnel meet training requirements (T-1).
2.18.1.1. The Squadron/CC or ARC/SGP will ensure that personnel (civilian and
military) performing audiograms are certified by an AF or DoD-equivalent course
that is CAOHC-approved (T-0). Reference Paragraph 2.9.2.20 and Attachment 3
for details.
2.18.1.2. The Squadron/CC or ARC/SGP will ensure new Air Force audiologists
attend a hearing conservation program-training course at USAFSAM within one year
of assignment to first duty station for active duty or within the first year of
employment for civilian audiologists (T-1). Contract audiologists who are hired to
perform hearing conservation program duties may attend training at USAFSAM or a
civilian equivalent in accordance with contract management policy.
2.18.2. Identify new personnel requirements to meet HCP mission needs (T-1).
2.19. Bioenvironmental Engineering (BE) will:
2.19.1. Perform noise surveys and dosimetry to quantify noise hazards as outlined in
Attachment 2 (T-0).
2.19.1.1. At the request of a pregnant worker’s attending provider, quantify specific
exposures if not previously quantified during routine or special assessments (T-1).
2.19.1.2. Ensure only qualified personnel ( A3.1 Certification) conduct the surveys
(T-0).
2.19.1.3. Document all results in DOEHRS-IH (T-0). Utilize the DOEHRS
Hazardous Noise Data Entry and Report Guide (DERG) for accurate input of data and
reports (T-2).
2.19.2. Work with Precision Measurement Equipment Laboratory and/or Biomedical
Engineering personnel to ensure calibration and certification of noise meters are
14 AFI48-127 26 FEBRUARY 2016
performed according to ANSI S1.4, Specification for Sound Level Meters (or current
ANSI standard) (T-0).
2.19.3. Complete the Occupational and Environmental Health Exposure Data for the
OEHWG, including the 8-hour TWA and required controls (T-2).
2.19.3.1. Ensure that resultant noise levels are below 85 dBA when using the
hierarchy of controls (T-0). If resultant noise levels are greater than or equal to 85
dBA then engineering controls should be the first method of control considered,
followed by administrative controls and PPE last (T-0).
2.19.3.1.1. Where engineering controls are undertaken, the design objective is to
reduce steady-state levels to below 85 dBA, regardless of personnel exposure
time, and to reduce impulsive noise levels to below 140 decibels (dB) peak sound
pressure level (SPL).
2.19.3.1.2. If engineering controls are not selected to control noise hazards, then
BE must document reason in DOEHRS-IH (reference the Noise DERG) (T-1).
2.19.3.2. Calculate at-the-ear exposure (T-1). Reference Attachment 4 for method
to estimate HPD attenuation.
2.19.3.2.1. Provide PH with a copy of the Certified Protective Equipment List,
which includes HPDs approved for SEG use and attenuation for each workplace
process (T-1).
2.19.3.2.2. Ear level exposure is recommended to be between 76 to 84 dBA for
an 8-hour exposure. Note: Care must be taken to avoid over protection.
Excessive attenuation may cause the worker distress resulting in non-compliance
with wearing the HPDs.
2.19.4. Provide PH and shop supervisors the results of noise surveys and dosimetry (T-
1). This information is to include hazard and required controls (i.e., engineering,
administrative, and/or HPD). This can be in the form of the certified PPE list if no
engineering controls are being used (reference the Noise DERG).
2.19.5. Approve HPDs for local use including local purchase items and HPDs for special
applications (T-1).
2.19.5.1. Verify the special need and ensure the device provides appropriate
attenuation (T-1).
2.19.5.2. Notify MAJCOM/SGPB and USAFSAM/OE if they have a special need
(T-2).
2.19.6. Assess the adequacy of all controls used to reduce noise exposures including
hearing protectors and evaluate industrial work areas where adverse hearing loss trends
are noted (T-1).
2.19.7. Assist with fitness and risk evaluations upon request of the provider, to include
hazardous noise exposures on and off duty (T-2).
2.19.8. Review facility and operations plans for new or modified facilities to ensure
noise exposure control is appropriately considered (T-1).
AFI48-127 26 FEBRUARY 2016 15
2.19.9. In conjunction with the shop supervisor, assess the feasibility of engineering
controls for hazardous noise equipment/areas (T-1).
2.19.10. Conduct work place assessments to support occupational illness/injury
investigations and claims for hearing loss (T-1).
2.19.11. Annually certify the audiometric testing environment with a Type I precision
sound level meter (SLM) with attached octave band analyzer and establish that
background octave band SPLs are not greater than the following (T-0):
2.19.11.1. For 500 Hertz (Hz), 27 dB.
2.19.11.2. For 1,000 Hz, 29 dB.
2.19.11.3. For 2,000 Hz, 34 dB.
2.19.11.4. For 4,000 Hz, 39 dB.
2.19.11.5. For 8,000 Hz, 41 dB.
2.19.12. When surveying the test environment use equipment conforming at least to the
Type I requirements of the latest approved ANSI Standard S1.4 and the order 3 extended
range requirements of the latest approved ANSI Standard S1.11, Specifications for
Octave-Band and Fractional Octave-Band Analog and Digital Filters (T-0).
2.19.13. Assign a RAC to all potentially hazardous noise areas and operations, IAW
DoDI 6055.01, DoD Safety and Occupational Health Program (T-0).
2.19.14. Coordinate any RAC 1, 2 or 3 with the installation safety office IAW AFI 91-
202, USAF Mishap Prevention Program, for inclusion into the installation Master Hazard
Abatement Plan (T-1).
2.19.15. Maintain a current inventory of all potentially hazardous noise areas and
operations to include, minimally, noise levels, RACs, and the types of control measures
used (T-0).
2.19.16. Provide technical assistance in initial monitoring, interpreting results, and
recommending controls when requested for facilities where recreational exposure to loud
music may occur (T-2).
2.20. Public Health (PH) will:
2.20.1. Manage and perform Occupational Hearing Conservation audiograms (except at
installations where separate Occupational Medicine Services are already established
outside of PH) (T-1). Place personnel identified as occupationally exposed to hazardous
noise (i.e., exposed to noise levels at or above 85 dB on an 8-hour TWA as identified by
BE survey and recommended by OEHWG) in a testing program that includes pre-
placement, periodic (at least annually), and termination audiograms (T-0). IAW DoDI
6055.12, personnel who infrequently or incidentally enter designated hazardous noise
areas are required to wear hearing protection but are not required to be enrolled in the
audiometric testing program. For ARC personnel assigned to workplaces which would
present them with occupational exposure to hazardous noise, an audiogram is not
required unless they are exposed to hazardous noise for more than 30 days per year. This
suspension from audiometric testing will not be viewed as a removal from the balance of
16 AFI48-127 26 FEBRUARY 2016
the protective requirements of the HCP. Exposed personnel will be included in hearing
conservation training, HPD issuance and fitting for work in hazardous noise
environments, and other elements of an effective HCP (T-0).
2.20.2. Track personnel on the HCP along with shop supervisors using the Occupational
Health Module in ASIMS (T-1). This includes monitoring occupational exam
compliance.
2.20.3. Ensure technicians who conduct testing are certified by an AF or DoD-equivalent
course that is CAOHC-approved (T-0). Training includes hands-on DOEHRS-HC
curriculum.
2.20.4. Perform, prior to every hearing test and every earplug fitting/assessment, a
lighted ear inspection (LEI) (T-2).
2.20.4.1. Performing a LEI helps to determine if cerumen removal or other treatment
is necessary to obtain an accurate audiogram and properly select, assess, and fit
earplugs.
2.20.4.2. Hearing conservationists are appropriately trained to perform LEI at the
Hearing Conservation course at USAFSAM.
2.20.4.3. All barriers (e.g., HPDs, hearing aids) must be removed before the LEI and
during the audiogram (T-2).
2.20.5. Provide standard instructions to individuals before testing (T-2).
2.20.6. Perform audiometric testing using the DOEHRS-HC software (T-0). Test Air
Force and Sister Service members using the appropriate DD Form 2215, Reference
Audiogram, and DD Form 2216, Hearing Conservation Data (T-0). Using the
appropriate forms avoids overuse of non-HC tests, which cannot be compared to a
baseline in order to monitor hearing changes.
2.20.7. Ensure that appropriate audiometric DOEHRS-HC data is forwarded to the
DOEHRS-DR, at the end of each testing day (T-0). Note: In the event of network issues,
export the records to either a shared network or disc and upload to the DR website when
available.
2.20.8. Perform audiometer calibration and functional checks (T-0).
2.20.8.1. Perform tests on calibrated audiometers (T-0). Reference Attachment 3.
2.20.8.2. Perform tests on audiometers that have received a functional and biological
operation check before each day's use as outlined in Attachment 3 (T-0). For further
specifications, reference DoDI 6055.12.
2.20.8.3. Ensure audiometers receive an annual electro-acoustic calibration by a
biomedical equipment technician (T-0). Reference Attachment 3.
2.20.9. Include pure-tone, air-conducted hearing threshold examinations of each ear at
the test frequencies of 500, 1,000, 2,000, 3,000, 4,000, and 6,000 Hz (T-0).
2.20.10. Conduct reference and pre-placement audiograms, and document on DD Form
2215 IAW the following (T-0):
AFI48-127 26 FEBRUARY 2016 17
2.20.10.1. All civilian personnel being considered for employment in an occupational
specialty or area that involves exposure to hazardous noise will receive a reference
audiogram, prior to but as close as possible to the actual date of anticipated noise
exposure, at no cost to the employee (5 CFR 339.303 & 339.304; 29 CFR 1910.95)
(T-0). Military personnel exposed to hazardous noise will receive a reference
audiogram prior to but not to exceed 30 days before the date of the workers’ initial
exposure to hazardous noise, including noise exposure at secondary training (T-0).
Exception: For all new officer and enlisted accessions who received a reference
audiogram at initial training, they will receive an annual audiogram if assigned to a
work area with hazardous noise. Note: Reference Attachment 3 for ‘reason’
selection.
2.20.10.1.1. The first valid hearing test administered is the reference audiogram.
The worker must be informed to avoid high levels of occupational or non-
occupational noise exposure during the 14-hour period preceding the examination
(T-0).
2.20.10.1.2. Hearing protectors will not be used to meet the 14-hour noise-free
requirement (T-0).
2.20.10.1.3. The officer accessions (e.g., Health Professional Scholarship
Program and ROTC students) who did not receive a reference audiogram at initial
training (no DD Form 2215 in DOEHRS-DR) will have an audiogram performed
by Public Health at the first duty location (T-1).
2.20.10.2. An Audiometric Case History (AF Form 1753, Hearing Conservation
Examination, Section I) will be completed on all reference audiograms (T-2). If
worse than H-1 hearing levels are noted, or if personnel answer “yes” to asterisked
questions, then a clinical examination is required, and the remainder of AF Form
1753 is to be completed (T-2).
2.20.10.3. Workers terminated from the HCP who subsequently return to hazardous
noise duties should have their current audiogram compared to their most recent
reference audiogram. If the current results do not indicate an STS, the most recent
reference audiogram serves as the reference audiogram. If an STS is present, use the
current audiogram to establish a new, type 3 reference audiogram (T-0).
2.20.10.4. Maintain a variety of earplugs and accomplish the initial earplug fitting
(T-0). Reference the fitting and dispensing section in Attachment 4 for details.
2.20.10.5. Consult an audiologist for workers who cannot be adequately fitted with
recommended HPD (T-0). Reference Attachment 4 for details.
2.20.11. Conduct annual audiograms and document on DD Form 2216 IAW the
following (T-0):
2.20.11.1. Personnel exposed to hazardous noise levels exceeding the standard
outlined in Attachment 2 will receive annual audiograms (T-0).
2.20.11.2. Examine the fit of pre-formed or the fit and condition of custom molded
earplugs at the time of the annual audiogram by having the individual place the HPD
in his/her ears as they would each day (T-1).

18 AFI48-127 26 FEBRUARY 2016
2.20.11.3. Document the date, type of HPD fitted, brand, noise attenuation provided,
and resultant noise level (request from BE) on a suitable document such as an SF 600,
Chronological Record of Medical Care, or an electronic equivalent, and place (or
upload) to the member’s medical record (T-1).
2.20.12. Complete a termination audiogram when a worker enrolled in the HCP stops
working in a designated hazardous noise area and will no longer be exposed as defined in
DoDI 6055.12. (T-0). Note: Personnel moving to other DoD jobs (i.e., PCSing,
PCAing) involving hazardous noise exposure with continued HCP enrollment need not
be given a termination audiogram unless they change DoD Components.
2.20.12.1. Military personnel exposed to hazardous noise will have a termination
audiogram documented before leaving military service. An audiogram conducted
within 12 months of separation/retirement can be considered a termination audiogram
(T-0). Note: Reference AFI 48-123, Medical Examination and Standards, for
guidance on the audiogram conducted for military personnel during the Separation
History and Physical Examination.
2.20.12.2. Follow the same follow-up and referral procedures as an annual
audiogram if an STS is identified on a termination audiogram (T-0).
2.20.13. Conduct and document HCP training on the SF 600 or the electronic equivalent
at every initial and annual audiogram (T-0), and place (or upload) to the member’s
medical record (T-1). HCP training covers:
2.20.13.1. The effects of hazardous noise on hearing, the purpose of hearing
protection, the proper use of hearing protection devices, the requirement to wear
HPDs when exposed to hazardous noise on duty, potential disqualification from
current duties as a result of hearing loss, and recommendations to wear hearing
protection off duty when exposed to hazardous noise (T-0).
2.20.13.2. The proper selection, fit, use, and care of personal hearing protectors and
demonstrating the ability to properly insert and fit HPDs. (T-0). This is to include
personnel requiring earmuffs.
2.20.13.3. Counselling on the interaction between HPDs interfacing with other forms
of PPE (T-1). Some types of PPE, such as eyewear, can create ill-fitting circumaural
HPDs if fit of all PPE is not evaluated collectively. Reference Attachment 4 for
details.
2.20.13.4. The purpose of audiometric testing, an explanation of the audiometric test
procedures (T-0), and counsel on the results of the tests (T-1).
2.20.14. Perform follow-up and referral procedures, as outlined below (T-0):
2.20.14.1. An STS includes a change in hearing threshold relative to the current
reference audiogram of an average of 10 dB or more at 2,000, 3,000, and 4,000 Hz,
in either ear. Age corrections will not be applied. Note: A single frequency 15 dB
shift at 1,000, 2,000, 3,000, or 4,000 Hz is considered an early warning flag with no
requirements for follow-up testing or referrals, but with a requirement to counsel the
patient and check hearing protection.
AFI48-127 26 FEBRUARY 2016 19
2.20.14.2. When an individual's audiogram shows an STS relative to the reference
audiogram in either ear the following must be accomplished (T-0):
2.20.14.2.1. If a negative STS (improved hearing threshold from reference
audiogram) is noted, a follow-up test will be administered the same day as the
periodic test (T-0). The results may be used to create a re-established reference
audiogram to reflect the improvement in pure tone acuity.
2.20.14.2.2. If a positive STS (decrease in hearing threshold from reference
audiogram) is noted, one or two noise-free (i.e., no hazardous noise exposure at
least 14 hours prior) follow-up tests are administered to confirm (T-0).
2.20.14.2.2.1. The noise-free follow-up tests may be administered on the
same day, but not on the same day as the periodic audiogram.
2.20.14.2.2.2. Follow-up testing must be done within 30 days of the annual
audiogram (T-0). If no follow-up tests are performed within 30 days after the
annual audiogram, then the annual audiogram is considered a PTS until
further evaluation by an audiologist is completed. For ARC members, follow-
up testing must be done within 60 days of the annual audiogram (T-1). If no
follow-up tests are performed within 60 days after the annual audiogram, then
the annual audiogram is a PTS until further follow-up is completed.
2.20.14.2.2.3. If the result of the first follow-up test does not indicate an STS,
a second follow-up test is not required, and the shift is a temporary threshold
shift (TTS). If the result of the first follow-up does indicate an STS, and a
second follow-up test is required IAW DoDI 6055.12, but the second follow-
up test does not indicate an STS, then the shift is also a TTS.
2.20.14.2.2.4. If an STS is noted on all required follow-up tests, then the STS
should be considered a PTS and patient referred to the provider or audiologist
for confirmation (T-0).
2.20.14.2.3. Ensure a provider or AF hearing conservationist performs LEI prior
to the noise-free audiogram (NFA) (T-1).
2.20.14.2.4. Refit the individual with hearing protection, instruct in its care, use,
and wear (T-0).
2.20.14.3. Refer all patients with a PTS or problem audiogram back to the
Occupational Health Consultant or to an audiologist (T-0). They determine what
further follow-up is required. Reference Table A6.1 in Attachment 6 to determine
the need for an AF HCDC/HCC evaluation.
2.20.14.4. An audiologist, an otolaryngologist, or other provider will perform an
evaluation to determine whether the STS is work-related or has been aggravated by
occupational noise exposure (T-0).
2.20.14.5. The worker is required to complete Section I of the AF Form 1753 prior to
medical referral for a PTS (T-1).
2.20.14.6. Installations may refer to other DoD, Tricare network or Veteran Affairs
(VA) audiology clinics. For installations that refer to non-AF audiologists, referrals
20 AFI48-127 26 FEBRUARY 2016
will include comprehensive audiometric testing sufficient to determine type and
degree of hearing loss, and possible causation to assist in determining work-
relatedness (T-0). Audiology reports will include any recommendations for hearing
aids, hearing protection, further medical referral, and include noise exposure history,
any known indicators to the cause of the hearing loss, and an interpretation of tests
results to explain the type and degree of hearing loss. The clinical outcomes will be
documented and properly coded in the electronic health record (T-0).
2.20.14.6.1. For referrals, the following procedures listed in paragraphs
2.20.14.6.1.1-2.20.14.6.1.6 will be conducted and the documents listed in
paragraph 2.20.14.6.1.7 and 2.20.14.6.1.8 will be provided to the audiologist
(T-0):
2.20.14.6.1.1. Pure tone air conduction test, under supra-aural earphones or
insert earphones, using pulsed tones for frequencies 250 Hz through 8,000 Hz
(to include 3,000 and 6,000 Hz).
2.20.14.6.1.2. Pure tone bone conduction test, using pulsed tones for
frequencies 500 through 4,000 Hz (to include 3,000 Hz).
2.20.14.6.1.3. Word recognition testing, under supra-aural earphones or insert
earphones, using electronically recorded lists presented at appropriate supra-
threshold levels.
2.20.14.6.1.4. Word testing using competing background noise if the patient
reports difficulty hearing/understanding in the presence of background noise.
2.20.14.6.1.5. Immittance measures to include tympanometry, and acoustic
reflexes obtained for both ipsilateral and contralateral conditions. Acoustic
reflex decay at 500-1,000 Hz should be accomplished if clinically warranted.
Note: All tests are to be performed unaided and with equipment calibrated per
the most current and applicable ANSI standards.
2.20.14.6.1.5.1. Proof of acceptable background sound pressure levels
measured in the audiometric test room. Note: This is required for network
audiologists.
2.20.14.6.1.5.2. Proof of current audiometer calibration. Note: This is
required for network audiologists.
2.20.14.6.1.6. Otoacoustic Emissions testing.
2.20.14.6.1.7. Copies of the most current DD Form 2215 and DD Form 2216
on record.
2.20.14.6.1.8. Copy of the AF Form 1753.
2.20.14.6.2. Track patients referred to HCDC/HCCs in conjunction with provider
to ensure findings and recommendations are reviewed and appropriate action
taken (T-2).
2.20.14.6.3. All audiology reports from non-DoD audiologists (i.e., Tricare
network or VA audiologists) will be sent securely and in compliance with
applicable regulations via fax, or email to the regional HCDC/HCC for AF
AFI48-127 26 FEBRUARY 2016 21
audiologist review and disposition (T-1). Note: DoD uniformed audiologists, and
DoD civilian and contract audiologists with appropriate HCP training are not
required to send to the regional HCDC/HCC for review and disposition.
2.20.14.7. Notification.
2.20.14.7.1. Notify an individual, in writing, within 21 calendar days when an
audiologist or a provider confirms the positive threshold shift is permanent (T-0).
Workers will also be informed, in writing, that their supervisors will be notified
that they have experienced a decrease in hearing (T-0).
2.20.14.7.2. Supervisors will be notified, in writing, within 10 calendar days after
individual notification that the worker has experienced a decrease in hearing (T-
0). The notification will not contain additional details without prior written
authorization by the worker IAW DoDI 6025.18, Privacy of Individually
Identifiable Health Information in DoD Health Care Programs, and DoD
6025.18-R, DoD Health Information Privacy Regulation (T-0). The supervisor
will be advised that any discussion of a worker’s hearing abilities with non-
authorized personnel is strictly prohibited (T-0).
2.20.14.8. Document and code the condition in the Electronic Health Record per
standards outlined in the Military Health System coding guidelines (T-0).
2.20.14.9. Re-establish the reference audiogram for a positive STS.
2.20.14.9.1. Replace the original reference audiogram with a new reference
audiogram when the medical evaluation confirms the STS noted during the annual
and follow-up audiograms is permanent (T-0). Replace with one of the following
options (as chosen by the reviewing audiologists or provider) for re-establishing
the reference audiogram (T-0):
2.20.14.9.1.1. Use the results of the most recent follow-up test.
2.20.14.9.1.2. Use the results of the audiology referral (if all pertinent
examiner and audiometer information are available for the DD Form 2215).
Diagnostic audiological threshold results are to be inputted manually at the
request of the audiologist or provider.
2.20.14.9.1.3. Conduct a separate hearing test on DD Form 2215 and use it as
a reference.
2.20.14.9.2. The original reference audiogram will be retained in the patient's
medical record (T-0).
2.20.14.10. Establish a revised reference audiogram when the hearing threshold
demonstrated on the annual and follow-up audiograms indicate significant
improvement over the existing reference audiogram (T-0).
2.20.15. Perform pre and post-deployment audiograms.
2.20.15.1. Perform pre-deployment audiograms (T-1). AF members may require pre-
deployment audiograms if they are deemed “at-risk” for hazardous noise exposure
during the deployment period (refer to remarks in deployment tasking line or
COCOM reporting instructions). Examples of higher risk deployments might include
22 AFI48-127 26 FEBRUARY 2016
Joint missions such as stability operations, humanitarian or emergency response
activities. Recommendations for follow-up and referrals will follow the same
procedures as outlined in this instruction.
2.20.15.2. After the deployment period, AF members who required a pre-deployment
audiogram will complete a post-deployment audiogram (DD Form 2216) within 30
days of returning to permanent assignment (T-1). Recommendations and follow-up
procedures for post-deployment audiograms (DD Form 2216) will follow the same
procedures as outlined in this instruction. Note: ARC members who deploy for 30
days or more are entitled to post-deployment follow-up care for 180 days upon return
to home station.
2.20.16. Ensure all completed HCP medical forms are included in the member’s
Electronic Health Record (EHR) (T-1).
2.20.17. Perform trend analysis for HCP compliance and outcome measures (i.e., test
compliance, STS and PTS rates, overall and/or workplace-specific data) (T-2). Use data
to determine management actions to improve the HCP (T-2). Compare observed trends
to the trends in the current “USAF Hearing Conservation Program, DOEHRS Data
Repository Annual Report” published by USAFSAM. Use data and trends to determine
management actions to improve the HCP (T-2). Investigate and provide re-education to
shops in which trends indicate compliance issues or negative hearing conservation
outcomes (T-2).
2.20.18. Conduct illness investigations related to reportable occupational hearing loss
and document in AFSAS (T-1).
2.20.18.1. Reporting to OSHA. Criteria for an OSHA-reportable STS are defined in
Attachment 1.
2.20.18.1.1. Report OSHA-reportable STS (i.e., PTS) in AFSAS (T-0). Case
must be closed within 7 calendar days of confirmation of the PTS by the
audiologist or overseeing provider IAW 29 CFR 1904.10 (T-0).
2.20.18.1.2. When an OSHA-reportable hearing loss occurs from an
instantaneous event (e.g., acoustic trauma from a one-time blast over pressure),
record the hearing loss as a work-related “injury” IAW OSHA-recommended
guidelines (T-0). Case must be closed within 7 calendar days of confirmation of
the PTS by the audiologist or overseeing provider (T-0).
2.20.18.1.3. Do not use age corrections for any hearing loss calculations (T-0).
2.20.18.1.4. Report the hearing loss only once unless an additional OSHA-
reportable loss of hearing is incurred (T-0).
2.20.19. Brief the OEHWG at least quarterly (or more frequently as directed) and
annually brief (or more frequently as directed) the ESOH Council on the HCP to include
unit compliance rates and unit-specific STS/TTS/PTS rates (T-2).
2.20.20. In consultation with OEHWG, conduct fitness and risk evaluations and forward
the completed AF Form 1754 to the appropriate medical record authority for inclusion in
the member’s medical record (T-2). Reference Attachment 5 for details on conducting
these evaluations.
AFI48-127 26 FEBRUARY 2016 23
2.20.21. Provide a semi-annual, or upon request, update to USAFSAM Epidemiology
Consultant Services Division (USAFSAM/PHR) with current contact information to
include HCP Point-of-Contact, mailing address, phone number and e-mail (T-2).
2.21. Biomedical Equipment Technician (or equivalent) will:
2.21.1. Ensure all calibrations and certifications are performed according to ANSI S1.4
and ANSI S3.1 or current ANSI standards (T-0).
2.21.2. Acoustically calibrate audiometers annually per 29 CFR 1910.95, Appendix E,
Acoustic Calibration of Audiometers (T-0).
2.21.3. Perform exhaustive calibrations every 2 years (T-0). Reference Attachment 3.
2.22. Installation level Hearing Conservation Program Manager (HCPM) will:
2.22.1. Ensure procedures are established to identify, schedule, and monitor all personnel
on the HCP (T-1).
2.22.2. Ensure only audiometers meeting the standards of the ANSI S3.6, Specification
for Audiometers, or the most current version of this ANSI standard are used in the HCP
(T-0).
2.22.3. Review the HCP for adequacy/appropriateness to protect workers from hazardous
noise (T-1). Include adequacy of education, audiogram completion rates, and adverse
hearing loss trends in relationship to workplaces/Air Force Specialty Codes/HPD usage,
etc. Note: The OEHWG is the proper forum to evaluate the program and address
concerns.
2.22.4. Trend and analyze DOEHRS-DR reports; attend and provide consultation on the
HCP for the OEHWG (T-2).
2.22.5. Ensure the most current version of DOEHRS-HC (or current HC software
application) is used, and technicians are adequately trained on the program (T-1).
2.22.6. Ensure hearing related fitness and risk evaluations are conducted and closed 45
days after determination that an evaluation is needed (T-2). Reference Attachment 5.
2.22.7. Ensure an efficient referral tracking mechanism is in place for audiograms
between providers in the MTF and any outside audiologist or agency (T-0).
2.23. Occupational Health Consultant (a flight surgeon or AF audiologist can serve this
function) will:
2.23.1. Review problem audiograms (defined in Attachment 1) and determine if further
evaluation is needed per DoDI 6055.12 and OSHA requirements (29 CFR 1910.95) (T-
0). If follow-up care is needed, then request HCDC/HCC consultations or medical
referrals for personnel who fall into the referral criteria at Table A6.1. in Attachment 6
(T-1).
2.23.2. Ensure medical recommendations restricting hazardous noise exposure are based
on (T-0):
24 AFI48-127 26 FEBRUARY 2016
2.23.2.1. Failure of the worker to meet medical standards as defined in AFI 48-123,
AFI 36-2101, Classifying Military Personnel (Officer and Enlisted), and 5 CFR 339
for job placement.
2.23.2.2. Inability of the worker to perform the essential functions of the job.
2.23.2.3. Probability of the worker endangering himself/herself or others if allowed
to work in a noise hazard environment. Consider the Risk Management (AFI 91-802)
matrix for assistance in the decision making process.
2.23.3. Ensure recommendations are made for reasonable accommodations that allow a
hearing-impaired worker to perform duties in a noise hazard environment without undue
risk to personal safety and health or the safety of others (T-1). Reference Attachment 5
for details on fitness and risk evaluations.
2.23.4. Ensure workers who are qualified for duty in hazardous noise areas, or processes
are able to perform essential job tasks and they are not a safety hazard to themselves or
others (T-1).
2.23.5. Attend and provide consultation to the OEHWG on HCP matters (T-2).
2.24. Flight Medicine or ARC provider will:
2.24.1. Consult with the audiologist or Occupational Health Consultant on all problem
audiograms and occupational hearing related referrals (T-1).
2.24.2. Develop knowledge of related OSHA and DoD guidance to ensure appropriate
audiometric follow-up and disposition occurs (as detailed in this instruction) (T-1).
2.24.3. Perform required periodic MSE and make clinical recommendations (T-0). A
regional HCDC/HCC audiologist can be consulted for appropriate clinical
recommendations.
2.24.4. Determine if workers possess the minimum physical abilities needed to perform
essential duties and responsibilities without undue risk to themselves or others (T-1).
2.24.5. Establish reference and periodic (annual and close scrutiny) evaluations to detect
signs and symptoms of noise induced hearing loss at an early stage to prevent progression
(T-1). The installation level HCPM is the point of contact.
2.24.6. In coordination with the installation level HCPM, initiate AF Form 1754 for
fitness and risk evaluations for personnel who exceed the H-1 profile and work in a
hazardous noise area, and make a medical recommendation (T-2). Determine the extent
of fitness and risk evaluation (T-2). Reference Attachment 5.
2.24.7. Determine whether a shift is related to an Ear, Nose and Throat (ENT) condition
(T-2). Advise worker of the condition and either treat or refer for treatment (T-2). If an
audiologist or provider determines the shift is not occupationally related (i.e., middle ear
infection) the MTF is not responsible for the referral or treatment costs for civilian
employees.
2.24.8. When indicated review, complete, and sign AF Form 1753 (T-2).
2.24.9. Complete Section II of the AF Form 1753, before a baseline audiogram is re-
established (T-2). An examination of the ears, to include a comprehensive audiological
AFI48-127 26 FEBRUARY 2016 25
evaluation as indicated, will be performed on patients with a PTS, individuals undergoing
a fitness and risk evaluation, getting a reference audiogram with worse than H-1 hearing
levels, or asymmetric hearing loss as defined in the Medical Standards Directory (T-1).
Record the results in Section II (T-2). The provider will note (T-2):
2.24.9.1. Condition of the external auditory canals and tympanic membranes.
2.24.9.2. Presence of middle ear disease and eustachian tube function.
2.24.9.3. Any condition that may interfere with the wear of HPD (permanently or
temporarily).
2.24.9.4. Any abnormality that might adversely affect the audiogram results.
2.24.10. Determine appropriate additional referral criteria as needed (T-2).
2.24.11. Document and code the condition in the Electronic Health Record per standards
outlined in the Military Health System coding guidelines (T-0).
2.24.12. Comply with Department of Labor Office of Workers’ Compensation Program
(OWCP) Hearing Loss Medical Requirements listed in Attachment 7 when completing
provider and audiologist reports (T-0).
2.24.13. Use the American Conference on Governmental Industrial Hygienists (ACGIH)
Threshold Limit Value Committee’s recommendation and restrict pregnant women after
20 weeks gestation from discharging firearms with larger than a .22 caliber round or
noise exposure greater than 115 decibels relative to the carrier (dBc) TWA and peak 155
dBc to protect fetus’ hearing (T-0). See Attachment 2 for further details.
2.24.13.1. Work with BE to appropriately characterize the work environment and to
recommend the sound levels that should be avoided (T-1).
2.24.13.2. Job rotation should be considered but not mandated for pregnant workers
who are exposed to hazardous noise after 20 weeks (T-2).
2.24.14. Track patients referred to HCDC/HCCs in conjunction with PH to ensure
findings and recommendations are reviewed and appropriate action taken (T-2).
2.25. Hearing Center of Excellence (HCE) will support AF HCP as appropriate within the
scope of their approved mission (T-2).
2.26. Hearing Conservation Diagnostic Center (HCDC) and Hearing Conservation Center
(HCC). Reference Attachment 6 for further details (e.g., referral criteria) and listing.
2.26.1. HCDC will provide a wide range of diagnostics and treatments in support of
clinical referrals (T-2).
2.26.2. HCC will provide diagnostic care in direct support of the HCP (T-2).
2.26.3. The regional AF HCDC/HCC will review all evaluations by non-DoD
audiologists (T-2).
2.26.4. AF HCDC/HCC will provide consultation and overview of referrals, so that
management and disposition of patients meet current AF standards (T-2).
2.27. Occupational and Environmental Health Working Group (OEHWG) will:
26 AFI48-127 26 FEBRUARY 2016
2.27.1. Ensure personnel who have occupational hazardous noise exposures that exceed
levels as identified in this instruction are monitored in the HCP (T-0).
2.27.2. Evaluate the effectiveness of the HCP by monitoring and reporting hazard
assessment and outcome metrics (T-0). Additional metrics to assist in measuring
program effectiveness will be determined by the OEHWG (T-2).
2.27.2.1. Noise-related metrics for evaluation are defined in DoDI 6055.05 and DoDI
6055.12.
2.27.2.2. Overall and workplace-specific outcome metrics to identify high-risk
occupations and areas, and to determine if further intervention is necessary are
outlined in DoDI 6055.12.
2.27.3. Review approved civilian hearing loss claims filed at the installation and
determine appropriate actions (e.g., focused education, increased audiometric monitoring,
and coordination) with Safety for increased compliance monitoring, or other actions
deemed necessary (T-1).
2.27.4. Document HCP decisions and recommendations in the OEHWG minutes (T-2).
MARK A. EDIGER
Lieutenant General, USAF, MC, CFS
Surgeon General
AFI48-127 26 FEBRUARY 2016 27
Attachment 1
GLOSSARY OF REFERENCES AND SUPPORTING INFORMATION
References
Title 5, CFR, Volume 1, Part 339, Medical Qualification Determinations, 1 January 2012
Title 10 USC Section 8013, Secretary of the Air Force, 16 January 2014
Title 29, CFR 1904.10, Recording and Reporting Occupational Injuries and Illness, 13 March
2015
Title 29, CFR 1910.95, Occupational Noise Exposure, 13 March 2015
Title 29, CFR 1910.145, Specifications for Accident Prevention Signs and Tag, 13 March 2015
Title 42 USC Section 4914, Development of Low-Noise-Emission Products, 7 January 2011
DoDI 4000.19, Support Agreements, 25 April 2013
DoDI 6025.18, Privacy of Individually Identifiable Health Information in DoD Health Care
Programs, 2 December 2009
DoDI 6055.05, Occupational and Environmental Health (OEH), 11 November 2008
DoDI 6055.01, DoDSafety and Occupational Health (SOH) Program, 14 October 2014
DoDI 6055.12, Hearing Conservation Program, 3 December 2010
DoDI 8910.01, Information Collection and Reporting, 19 May 2014
DoD 6025.18-R, DoD Health Information Privacy Regulation, 24 January 2003
MIL-STD-1474E, Department of Defense Design Criteria Standard Noise Limits, 15 April 2015
AFI 33-360, Publications and Forms Management, 25 September 2013
AFI 36-2101, Classifying Military Personnel (Officer and Enlisted), 25 June 2013
AFI 41-210, Tricare Operations and Patient Administration Functions, 6 June 2012
AFI 48-101, Aerospace Medicine Enterprise, 8 December 2014
AFI 48-123, Medical Examination and Standards, 5 November 2013
AFI 48-145, Occupational and Environmental Health Program, 22 July 2014
AFI 63-101/20-101, Integrated Life Cycle Management, IC 2, 23 February 2015
AFI 65-601, Volume 1, Budget Guidance and Procedures, 16 August 2012
AFI 90-801, Environment, Safety, and Occupational Health Council, 25 March 2005
AFI 90-802, Risk Management, 11 February 2013
AFI 91-202, The USAF Mishap Prevention Program, 24 June 2015
AFI 91-203, Air Force Consolidated Occupational Safety Instruction, 15 June 2012
AFMAN 33-363, Management of Records, 1 March 2008
AFMAN 36-2622 V5, Personnel Concept III (Civilian) End User’s Manual, 1 March 1997
28 AFI48-127 26 FEBRUARY 2016
AFMAN 48-146, Occupational and Environmental Health Program Management, 9 October
2012
AFPAM 90-803, Risk Management (RM) Guidelines and Tools, 11 February 2013
AFPD 48-1, Aerospace Medicine Enterprise, 23 August 2011
AFPD 90-8, Environment, Safety and Occupational Health Management and Risk Management,
2 February 2012
AFVA 48-101, Caution-Hazardous Noise Area-May Cause Hearing Loss-Hearing Protection
Required, 1 November 1996
AFVA 48-103, Caution-Hearing Protection Must Be Worn When This Equipment is in
Operation Label (Issued by Sheet, 12 Labels per Sheet), 1 November 1996
AFVA 48-104, Caution-Hearing Protection Must Be Worn When This Equipment is in
Operation Label (Issued by Sheet, 25 Labels per Sheet), 1 November 1996
AFVA 48-150, Caution-Hearing Protection Must Be Worn When This Equipment is in
Operation Label (3 ½ x 5), 1 February 2001
ANSI S3.2 (R2009) Method for Measuring the Intelligibility of Speech over Communication
Systems.
ANSI/ASA S1.4-2014, Sound Level Meters.
ANSI S1.11-2004 (R2009), Octave-Band and Fractional Octave-Band Analog and Digital
Filters.
ANSI S1.25-1991 (R2007), American National Standard Specifications for Personal Noise
Dosimeters.
ANSI S3.1-1999 (R2008), Maximum Permissible Ambient Noise Levels for Audiometric Test
Rooms.
ANSI S3.6-2010 (or most current edition), Specification for Audiometers.
ANSI/ASA 12.6-2008, Methods for Measuring the Real-Ear Attenuation of Hearing Protectors.
ANSIASA 12.68-2007 (R2012), Methods of Estimating Effective A-Weighted Sound Pressure
Levels When Hearing Protectors are Worn.
ANSI S12.42-2010, Methods for the Measurement of Insertion Loss of Hearing Protection
Devices in Continuous or Impulsive Noise Using Microphone-in-Real-Ear or Acoustic Test
Fixture Procedures.
ANSI/ASA S12.65-2006 (R2011), American National Standard for Rating Noise with Respect to
Speech Interference.
Environmental Protection Agency Report 550/9-74-004, Information on Levels of Environmental
Noise Requisite to protect Public Health and welfare with an Adequate Margin of Safety.
American Conference of Governmental Industrial Hygienists (ACGIH) TLVs and BEIs, Based
on the Documentation of the Threshold Limit Values for Chemical Substances and Physical
Agents & Biological Exposure Indices, Latest Edition.

AFI48-127 26 FEBRUARY 2016 29
The Medical Standards Directory at
https://kx2.afms.mil/kj/kx4/FlightMedicine/Documents/Medical Standards Directory (MSD)
DOEHRS Hazardous Noise Data Entry and Report Guide (DERG)
Prescribed Forms
AF Form 1672, Hearing Conservation Diagnostic/Center Referral
AF Form 1753, Hearing Conservation Examination
DD Form 2215, Reference Audiogram
DD Form 2216, Hearing Conservation Data
DD Form 2217, Biological Audiometer Calibration Check
Adopted Forms
AF Form 55, Employee Safety and Health Record
AF Form 422, Notification of Air Force Member’s Qualification Status
AF Form 847, Recommendation for Change of Publication
AF Form 1754, Job Capability and Safety Analysis
SF 600, Chronological Record of Medical Care
SF 600e, DOEHRS-HC Hearing Loss Referral
Abbreviations and Acronyms
ACGIH—American Conference of Governmental Industrial Hygienists
AF—Air Force
AFI—Air Force instruction
AFMAN—Air Force manual
AFMC—Air Force Materiel Command
AFMSA—Air Force Medical Support Agency
AFOSH—Air Force Occupational and Environmental Safety, Fire Protection, and Health
AFPAM—Air Force pamphlet
AFPD—Air Force policy directive
AFRL—Air Force Research Laboratory
AFSAS—Air Force Safety Automated System
AFSEC—Air Force Safety Center
ANG—Air National Guard
ANR—Active Noise Reduction
ANSI—American National Standards Institute
30 AFI48-127 26 FEBRUARY 2016
AR—Air Reserve
ARC—Air Reserve Component
ASIMS—Aeromedical Services Information Management System
BE—Bioenvironmental Engineering
BEI—biological exposure indices (from ACGIH)
CAOHC—Council for Accreditation of Occupational Hearing Conservation
CFR—code of federal regulations
dB—decibel
dBA—decibels A-weighted
dBc—decibels relative to the carrier
DERG—Data Entry and Report Guide
DoD—Department of Defense
DoDI—Department of Defense instruction
DOEHRS-DR—Department of Defense Occupational Environmental Health Readiness System-
Data Repository
DOEHRS-HC—Department of Defense Occupational Environmental Health Readiness System-
Hearing Conservation
DOEHRS-IH—Department of Defense Occupational Environmental Health Readiness System-
Industrial Hygiene
ECL—equivalent continuous level
ENT—ear, nose, and throat, usually refers to an otolaryngologist
ESOH—Environment, Safety and Occupational Health
HAF—Headquarters Air Force
HCC—hearing conservation center
HCDC—hearing conservation diagnostic center
HCP—Hearing Conservation Program
HCPM—Hearing Conservation Program Manager
HIPAA—Health Insurance Portability and Accountability Act
HPD—hearing protection device
HPW—Human Performance Wing
HQ—headquarters
Hz—hertz
JSA—Job Safety Analysis
AFI48-127 26 FEBRUARY 2016 31
LEI—lighted ear inspection
MAJCOM—major command
MSD—Medical Standards Directory
MSE—Medical Surveillance Examination
MTF—medical treatment facilities
NFA—noise-free audiogram
NIOSH—National Institute for Occupational Safety and Health
NSN—national stock number
NRR—noise reduction rating
OEH—Occupational and Environmental Health
OEHWG—Occupational Environmental Health Working Group
OSHA—Occupational Safety and Health Administration
OWCP—Department of Labor Office of Workers’ Compensation Program
PA—Privacy Act
PCA—permanent change of assignments
PCS—permanent change of station
PDO—publishing distribution office
PESHE—Programmatic Environmental, Safety and Health Evaluations
PH—Public Health
PPE—personal protective equipment
PTS—permanent threshold shift
RAC—Risk Assessment Code
RH—Human Effectiveness Directorate
RHCB—Battlespace Acoustics Branch
RMU—Reserve Medical Unit
SEG—similar exposure group
SG—Surgeon General
SG3P—Chief, Aerospace Medicine Policy and Operations
SG3PB—Bioenvironmental Engineering Branch
SG3PM—Public Health and Preventive Medicine Branch
SORN—System of Records Notices
SLM—sound level meter
32 AFI48-127 26 FEBRUARY 2016
SPL—sound pressure level
Std—Standard
STS—significant threshold shift
TLV—threshold limit values (from ACGIH)
TTS—temporary threshold shift
TWA—time-weighted average
USAF—United States Air Force
USAFSAM—United States Air Force School of Aerospace Medicine
USAFSAM/OE—United States Air Force School of Aerospace Medicine Occupational and
Environmental Health Department
USAFSAM/PH—United States Air Force School of Aerospace Medicine Public Health
USAFSAM/PHR—United States Air Force School of Aerospace Medicine Epidemiology
Consult Services Division
USC—United States Code
Terms
Air Force Certified Hearing Conservationists—Personnel that complete the USAFSAM
Hearing Conservation Certification Course and are trained IAW the Council for Accreditation in
Occupational Hearing Conservation to perform audiometric testing in support of the Air Force’s
Hearing Conservation Program. The USAFSAM Hearing Conservation Certification must be
renewed every 5 years.
Annual Audiogram—An audiogram performed at least annually (also called periodic
audiogram).
Appointing Official—Personnel officer or official authority to make management decisions
concerning hiring, placement, accommodation, and termination of employees.
Audiogram—The measurement of a worker’s hearing sensitivity expressed in decibels as a
function of frequency. Data are reported in graphic or numeric form.
Audiologist—A clinician, researcher, or consultant, specializing in the preservation, evaluation,
and rehabilitation of hearing.
Close Scrutiny Audiogram—Frequently administered audiograms used to closely monitor a
worker or group. When, on whom, and how often to perform scrutiny exams is determined by
the credentialed health care provider (provider, nurse practitioner, physician assistant or
audiologist) who performs occupational health examinations, or as directed by the OEHWG.
Criterion Level—The sound level allowed for an 8-hour exposure, used as the basis for
measurement of a noise standard. For the Air Force the criterion level is 85 dBA.
Department of Defense Occupational and Environmental Health Readiness System-DR—
DOEHRS-HC data collection, retrieval and reporting site; used to submit, retrieve, and report
DOEHRS-HC data; location for downloading updated DOEHRS-HC lookup tables.
AFI48-127 26 FEBRUARY 2016 33
Department of Defense Occupational Environmental Health Readiness System-HC—An
automated audiometric system used by the military services for hearing conservation purposes.
Exchange Rate (or doubling rate)—The time-intensity exchange rate for determining length-
intensity of equivalent exposure levels. The AF uses a 3-dB exchange rate. Reference
Hazardous Noise Surveillance Requirements.
Fitness and Risk Evaluation—Evaluations performed by medical and safety professionals for
the purpose of determining a worker’s ability to perform specific job tasks (fitness) and the
likelihood of harm, either to the worker or others (risk), in relation to anticipated workplace
exposures and job demands. In the USAF HCP, fitness and risk evaluations are the processes
used to evaluate workers who, if placed at work in hazardous noise, may not be able to perform
essential duties adequately or may pose a health or safety risk to themselves or others.
H Profile—Hearing Profile threshold criteria (H-1 through H-4) are defined in AFI 48-123 and
the Medical Standards Directory. This criterion is used to identify workers for further evaluation
to determine if they are able to capably and safely perform their job in a hazardous noise
environment.
Hearing Conservation Program Manager (HCPM)—An individual appointed by the MTF
Commander or Ground RMU/GMU Commander for ARC. The HCPM, usually a credentialed
provider, is responsible for managing all aspects of the HCP while ensuring OSHA/DoD/AFI
compliance. However, HCPM access in DOEHRS-DR is often assigned to the senior NCO of
PH.
Hearing Conservationist—military or civilian member that is CAOHC trained. Reference
Attachment 3.
Impulsive or Impact Noise—A short burst of acoustic energy consisting of either a single burst
or a series of bursts. The pressure-time history of a single burst includes a rapid rise to a peak
pressure followed by a somewhat lower decay of the pressure envelope to ambient pressure. A
series of impulses may last longer than 1 second.
Negative Threshold Shift (Lower Hearing Threshold than Reference)—Same criteria as STS
calculations except negative shift represent improved hearing levels.
Noise—Free Audiogram (NFA)—An audiogram performed after a worker has not been
exposed to noise greater than 72 dBA or impulsive noise greater than 120 dB peak for a
minimum specified amount of time. (e.g., 14-hour NFA, requires a minimum of 14 hours noise-
free prior to the test). HPDs cannot be used to reach this noise-free status. All noise-free follow-
up audiograms must be completed within 30 days of the annual audiogram.
Occupational Health Consultant—A provider, usually a Flight Surgeon that serves as
consultant to primary care teams for operational health concerns, including review of problem
audiograms, to determine if further testing is required before disposition. An audiologist can
serve as a consultant for audiology/hearing conservation review/disposition concerns.
OSHA Reportable Hearing Loss—If a worker’s current audiogram reveals that the worker has
experienced a work-related STS (as defined) in one or both ears and the worker’s total hearing
level is 25 dB or more above audiometric zero (averaged at 2000, 3000, and 4000 Hz) in the
same ear(s) as the STS, you must report the case to OSHA via AFSAS within 7 calendar days.
Figure A1.1. Decision Tree for Reporting Hearing Loss.
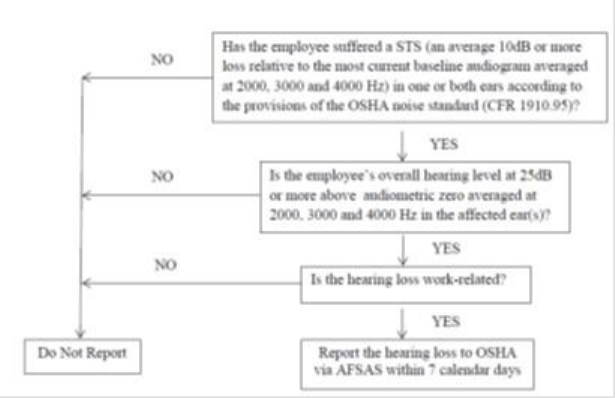
34 AFI48-127 26 FEBRUARY 2016
Otoscopic Examination (lighted ear inspection)—The act of viewing the external auditory
canal to the tympanic membrane. This exam is accomplished with the use of an otoscope.
Peak Pressure Level—The maximum absolute level, in dB, achieved for any specified time
interval.
Permanent Threshold Shift (PTS)—Any STS found on monitoring audiometry which is still
present after required follow-up 14-hour NFAs is considered a PTS. An STS on an annual
audiogram is also considered a PTS if follow-up testing is not conducted in the specified time.
Positive Threshold Shift (Higher Hearing Threshold than Reference)—Same criteria as STS
calculations. Positive shifts represent poorer hearing levels.
Potential Hazardous Noise—Exposure to steady-state noise having an 8-hour TWA noise level
greater than or equal to 85 dBA, or exposure to impulsive/impact noise levels greater than 140
dB peak SPL, regardless of duration.
Potentially Hazardous Noise Area—Any area where workers are likely to be exposed to noise
levels equal to or greater than an 8-hour TWA of 85 dBA, or where impulsive noise levels
exceed 140 dB peak SPL.
Pre-placement Audiogram—All persons entering employment in hazardous noise (greater than
or equal to an 8-hour TWA of 85 dBA, the OSHA limit) will receive an audiogram prior to
beginning work. The results of the pre-placement audiogram, if meeting the requirements of a
reference audiogram, may be used as the reference audiogram.
AFI48-127 26 FEBRUARY 2016 35
Problem Audiograms—Audiograms that show large differences in hearing thresholds between
the two ears, audiograms that show unusual hearing loss configurations that are atypical of noise
induced hearing loss, and/or audiograms with thresholds that are not repeatable. A HCDC/HCC
audiologist can be consulted to review problem audiograms.
Reference Audiogram—An audiogram used as a baseline to compare subsequent audiograms
against to determine if hearing loss has occurred. All persons entering employment in hazardous
noise (greater than or equal to an 8-hour TWA of 85 dBA, the OSHA limit) should receive a pre-
placement audiogram that should be used as the reference audiogram. Also called baseline
audiogram by OSHA.
Sound Level (Noise Level)—The weighted sound pressure level measured by the use of a meter
with characteristics and weighting A. B. or C. as specified in ANSI S1.4. The weighting must be
indicated; otherwise, the A-weighting is understood.
Sound Pressure Level—The sound pressure level of a sound, in dB, which is 20 times the
logarithm to the base ten of the ratio of the pressure of this sound to the reference pressure of 20
microPascals (uPa) (20 microNewton/m2) (2 X 10
-4
microbar).
Speech Interference Level—The arithmetic average of the sound pressure levels, in dB, of a
noise in the four octave bands of center frequency 500, 1,000, 2,000, and 4,000 Hertz.
Significant Threshold Shift (STS) —A change in hearing thresholds relative to the reference
audiogram. An average change of 10 dB or more at 2,000, 3,000, and 4,000 Hz in either ear,
according to CFR 1910.95. That is, if the sum of the shifts at 2,000, 3000, and 4,000 Hz equals
or exceeds 30 dB in either ear, an STS has occurred. Use of age corrections will NOT be applied
when determining STS. Note: OSHA terminology is standard threshold shift.
Temporary Threshold Shift (TTS) —A temporary loss of hearing due to noise exposure. Any
positive STS that is not confirmed by the noise free follow-up test is considered a TTS, unless
there is a resolved medical condition.
Termination Audiogram—A hearing test administered and recorded on DD Form 2216 when a
worker discontinues employment involving hazardous noise exposure as defined in DoDI
6055.12. A Termination Audiogram shall be accomplished when a hazardous noise exposed
worker, who has been included on the HCP, separates or retires from military/civil service.
Individuals who are PCSing, PCAing, do not require a Termination Audiogram if a periodic
audiogram was completed within 12 months.
Threshold Level—A sound level below, which exposures are not included in dose calculations
or measurements. For this standard, the threshold is 80 dBA.
Time-Weighted Average (TWA)—The time-weighted average sound level or exposure for an
8-hour workday and 40-hour workweek.
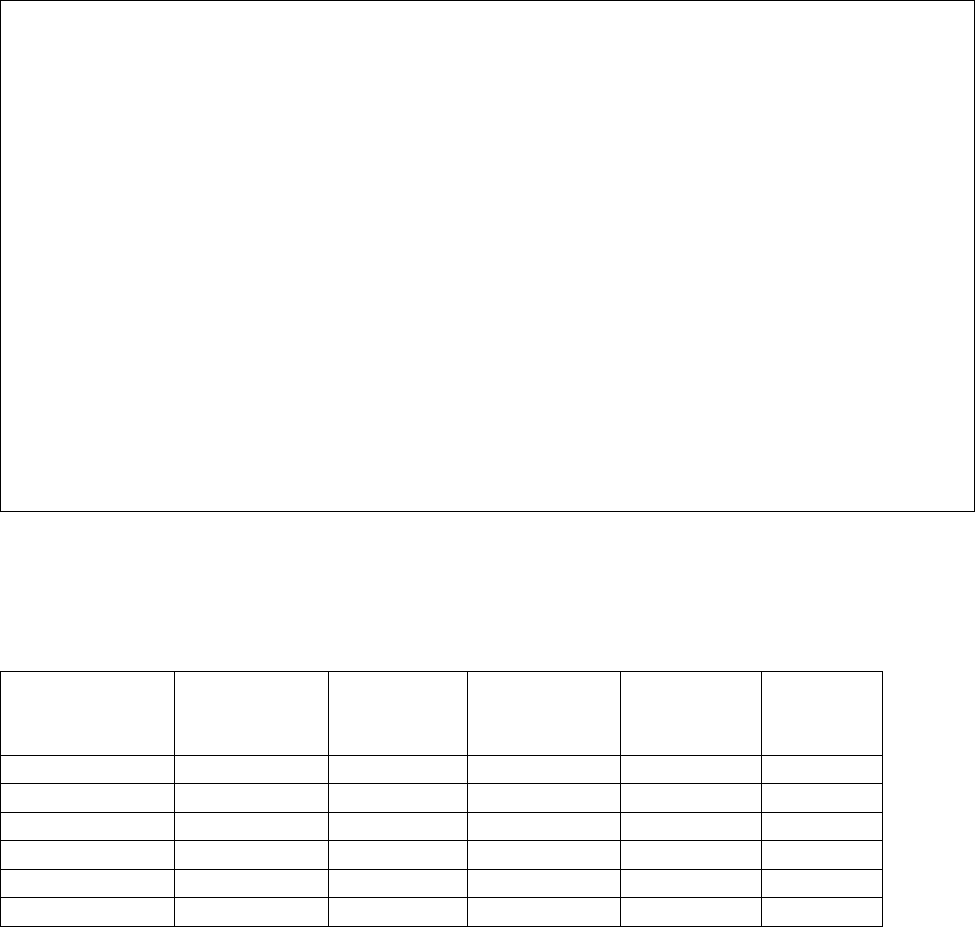
36 AFI48-127 26 FEBRUARY 2016
Attachment 2
HAZARDOUS NOISE SURVEILLANCE
A2.1. Noise Exposure Limits on Hearing. The occupational and environmental exposure limit
(OEEL) is the most appropriate limit adopted from established, recognized standards (e.g., latest
edition of the TLV® Booklet published annually by the American Conference of Government
Industrial Hygienists, 29 CFR 1910.1000 Tables Z-1, Z-2, and Z-3 and 40 CFR 141) for noise
and is intended to prevent damage to the hearing of exposed personnel. These noise exposure
limits are sound levels and durations to which nearly all workers may be exposed without
permanent adverse effect on their ability to hear and understand normal speech.
Table A2.1. Health Protection Criteria
Hearing Protection*
85 dBA, 8-hours or equivalent exposure times (reference Table A2.2.)
Criterion level
85 dBA
Exchange rate
3 dB
Threshold level
80 dBA
Maximum level
115 dBA
Impulsive Noise
L
IAeq100ms
=85 dBA. Reference MILSTD 1474E Appendix B for
impulsive noise requirements.
Whole Body Effects*
No octave or one-third octave band level above 145 dB for
frequencies from 1 Hz to 40 kHz
Ultrasound*
Reference Table A2.3.
Exposure to Music
Patrons
Leq.2h < 90 dBA
Employees*
Same as occupational standard
Air Force Musicians*
Same as occupational standard
* Based on recommendations from the Threshold Limit Values for Chemical Substance and Physical Agents &
Biological Exposure Indices published by the American Conference of Governmental Industrial Hygienists; the
current edition of this annual publication will be applied. Applies for on and off duty exposure.
A2.1.1. Continuous or Intermittent Exposures. The duration of unprotected noise exposure
per day will not exceed the values specified in Table A2.2 for the levels indicated for
continuous exposure.
Table A2.2. Limiting Values for Unprotected Noise Exposures*.
Sound Level
(dBA)
Time
(minutes)
Sound
Level
(dBA)
Time
(minutes)
Sound level
(dBA)
Time
(minutes)
Over 115
Forbidden
115
0.5
102
9.5
89
190
114
0.6
101
12
88
240
113
0.7
100
15
87
302
112
0.9
99
19
86
381
111
1.2
98
24
85
480
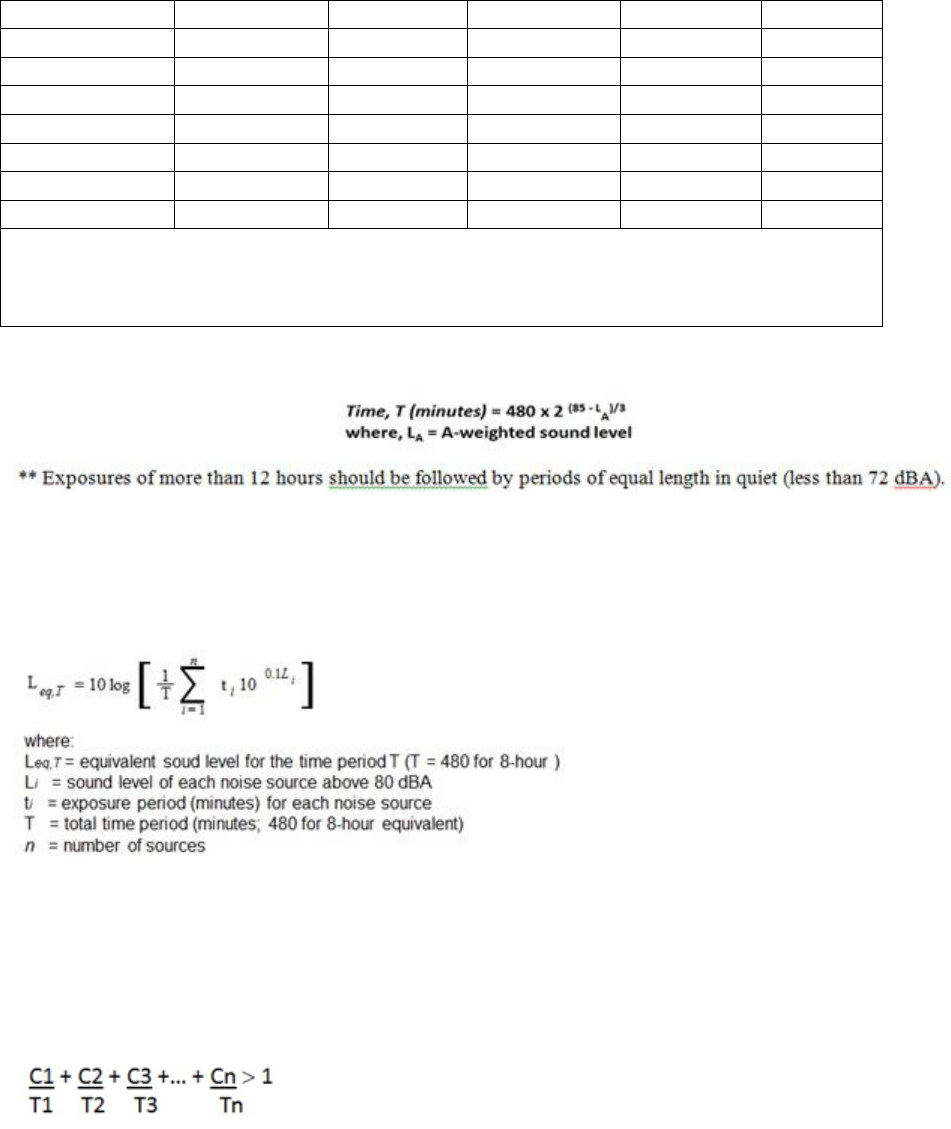
AFI48-127 26 FEBRUARY 2016 37
110
1.5
97
30
84
605
109
1.9
96
38
83**
762
108
2.4
95
48
82**
960
107
3.0
94
60
81**
1210
106
3.8
93
76
80**
24 Hours
105
4.7
92
95
Below 80
No limit
104
6.0
91
120
103
7.5
90
151
* The A-weighted sound level is used to assess hearing damage risk due to noise exposure; for engineering
noise control, other measures are required. The limiting duration of exposure at any noise level equal to or
less than 115 dBA is determined from the equation at Figure A2.1.:
Figure A2.1. Duration of Exposure Calculation.
A2.1.1.1. If exposures to two or more levels occur in one day, their combined effect
should not exceed an 8-hour equivalent continuous level, Leq, 480 min, of 85 dB, given
by the equation in Figure A2.2:
Figure A2.2. Calculating Equivalent Sound Level.
A2.1.1.2. This is equivalent to summing the fractions of the actual time of exposure to
the allowable time of exposure. If this value exceeds one (1), the combined exposure
should then be considered to exceed the standard. This may also be expressed
mathematically as:
Figure A2.3. Unity Calculation.
A2.1.1.3. The C values are the actual exposure times to a given level; the T values are
the times allowed at those levels by Table A2.3. All occupational noise exposures above
the threshold level of 80 dBA will be used in the above equations IAW OSHA 29 CFR
1910.95.
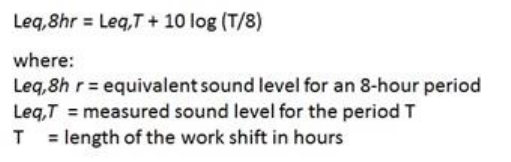
38 AFI48-127 26 FEBRUARY 2016
A2.1.1.4. For work shifts other than 8-hour periods, the measured average noise
exposure should be adjusted to an 8-hour equivalent exposure level using Figure A2.4:
Figure A2.4. Calculating 8-hour Equivalent Sound Level.
A2.1.2. Impulsive or Impact Exposures. Unprotected personnel will not be exposed to
impulsive or impact noise. Reference MILSTD 1474E for impulsive noise requirements.
A2.1.3. Hazardous Noise Areas. A potentially hazardous noise area will be clearly
identified by signs located at entrances to, or the borders of, the area. Signs will be designed
according to the guidelines in DoDI 6055.12, and will have the following message:
CAUTION
HAZARDOUS NOISE AREA
HEARING PROTECTION REQUIRED
A2.1.3.1. Signs and/or decals will describe (in words or with other visual symbols) the
potential hazard and the required protective measures (e.g., “Danger”, “Hazardous
Noise”, “Hearing Protection Required When in Operation”). Such wordings as "When
machines are operating" or "Within 25 feet of operating band saw” may be added at the
bottom of the caution sign to accurately identify the noise hazard area.
A2.2. Noise Exposure Limits on Whole Body Effects. At certain high sound pressure levels,
exposed persons may suffer adverse effects, which do not involve the hearing organs. Whole
body limits are designed to prevent these effects.
A2.2.1. No octave or one-third octave band level may exceed 145 dB for frequencies in the
range of 1 Hz through 40 kHz, and the overall sound pressure level cannot exceed 150 dB
(unweighted). There are no time limits for exposures below these levels. However,
protecting hearing requires adherence to the hearing protection limits mentioned above, in
addition to the ultrasonic evaluation requirements mentioned in the next paragraph, to protect
against non-auditory effects of noise; this applies regardless of any hearing protection used.
A2.2.2. The impact of workplace equipment or other workplace conditions causing
ultrasonic noise exposures will be evaluated. The limits specified in DoDI 6055.12 and the
latest version of ACGIH Threshold Limit Values (TLV) for Chemical Substances and
Physical Agents should be used. Note these limits are designed to protect hearing. They
apply at the ear, and hearing protective devices can be used to meet these limits.
Consultation with USAFSAM/OE may be required in measuring or evaluating ultrasonic
noise.
AFI48-127 26 FEBRUARY 2016 39
Table A2.3. Exposure Guidelines for Upper Sonic and Ultrasound Noise*.
One-Third Octave-Band SPL (dB re: 20 microPascals (μPa))
Mid-Frequency of
Third Octave Band
(kHz)
Ceiling Values
8-Hour TWA
10
105
A
88
A
12.5
105
A
89
A
16
105
A
92
A
20
105
A
94
A
25
110
--
31.5
115
--
40
115
--
50
115
--
*ACGIH, 2010 TLVs and BEIs. These recommended limits (set at the middle frequencies of the one-
third octave bands from 10 kHz to 50 kHz) are designed to prevent possible hearing loss caused by the
subharmonics of the set frequencies, rather than the ultrasonic sound itself. (Also, reference most current
version of American Conference of Governmental Industrial Hygienists for updates). Consultation with
appropriate DoD Component technical centers may be required in measuring or evaluating equipment
producing those levels.
A
Subjective annoyance and discomfort may occur in some individuals at levels between 75 and 105 dB
for the frequencies from 10 kHz to 20 kHz especially if they are tonal in nature. Hearing protection or
engineering controls may be needed to prevent subjective effects. Tonal sounds in frequencies below 10
kHz might also need to be reduced to 80 dB.
A2.2.3. Pregnant Workers. Fetal noise is a controversial topic with limited research on
which to base exposure guidelines for pregnant women. A few studies suggest noise is a
potential hazard; however, these studies provide insufficient evidence to establish firm fetal
noise protection guidelines. There is evidence to suggest that noise exposure in excess of a
C-weighted, 8-hour Leq,T of 115 dBC or a peak exposure of 155 dBC to the abdomen of
pregnant workers, beyond the fifth month of pregnancy, may cause hearing loss in the fetus
(reference 2.23.12). Job rotation or modification of job tasks should be considered to create
the safest and healthiest environment for pregnant workers and their unborn children.
However, concern for safety and health should not lead to inappropriate actions that may
constitute unlawful discrimination against pregnant women in the workplace.
A2.2.3.1. Job rotation should be considered but not mandated for pregnant workers who
are exposed to hazardous noise after 20 weeks. Using job rotation for 20+ week
pregnancies is highly recommended but not mandated for workers having an equivalent
continuous level (ECL) at or above 100 dBA unprotected exposure.
A2.2.3.2. Working in impulsive or impact noise environments, requiring hearing
protection (e.g., firing ranges, EOD detonations, etc.), should be avoided by pregnant
workers.
A2.2.4. If ototoxic chemicals are present in hazardous noise areas, be aware the chemicals
may act in an additive or synergistic mode to increase the risk of hearing loss.
40 AFI48-127 26 FEBRUARY 2016
A2.2.5. No impulsive noise exposure will exceed 190 dB peak unless an analysis of non-
auditory damage risk is conducted to include but not limited to blast lung injury. No
impulsive noise exposure will exceed 197 dB peak.
A2.3. Noise Exposure Limits on Job Performance. Noise exposure limits in this section are
provided to maintain effective job performance. These limits should be used as design
recommendations in the construction of new facilities or to address concerns or correct problems
arising from present conditions that interfere with accomplishing current tasks or operations.
A2.3.1. Quality of Person-to-Person Communication. The data shown in Table A2.4
provides ranges of sound levels and the corresponding routine communication capability for
several situations. When evaluating speech interference near small arms areas, or other areas
where hearing protection is worn, the attenuation of the hearing protection will be taken into
account.
Table A2.4. Quality of Person-to-Person Voice Communication*.
Voice Levels
Noise Level
(dBA)
Normal
Voice
Raised
Voice
Shouting
Telephone Use
40 to 50
Satisfactory
to 30 feet
Satisfactory
50 to 60
Satisfactory
to 6 feet
Satisfactory
Satisfactory
60 to 70
Satisfactory
to 3 feet
Satisfactory
to 6 feet
Satisfactory to slightly
difficult
70 to 80*
Satisfactory
to 1 foot
Satisfactory
to 3 feet
Slightly difficult
80* to 90
Satisfactory
to 1 foot,
Slightly difficult
Difficult
90 to 95
Slightly
difficult to
2 feet
Slightly difficult
to 3 feet
Very Difficult
Above 95
Slightly difficult
to 1 foot
Unsatisfactory
*Noise exposure limits may be exceeded by a combination of noise plus voice.
A2.3.2. Office and Work Space. Noise measurements made for comparing noise in an office
with these criteria should be done with the office in normal operation, but with no one talking
at the location where speech communication is being evaluated. Background noise with the
office unoccupied should be lower by 5 to 10 dBA. Acceptable levels are at Table A2.5 and
Table A2.6.
AFI48-127 26 FEBRUARY 2016 41
Table A2.5. Noise Levels for Offices*.
Range of Levels
(dBA)
Communication Environment
30 to 40
Very quiet office, telephone use satisfactory, suitable for large conferences.
40 to 45
Quiet office, satisfactory for conferences at a 15 foot table; telephone use
satisfactory; normal voice 10 to 30 feet.
45 to 50
Satisfactory for conferences at a 6 to 8 foot table; telephone use satisfactory;
normal voice 6 to 12 feet
50 to 60
Satisfactory for conference at 4 to 5 foot table; telephone use occasionally
slightly difficult; normal voice 3 to 6 feet; raised voice 6 to 12 feet.
60 to 65
Unsatisfactory for conference of more than two or three people; telephone
use slightly difficult; normal voice 1 to 2 feet; raised voice 3 to 6 feet.
Above 65
Very noisy; office environment unsatisfactory; telephone use difficult.
Table A2.6. Noise Levels for Work Spaces*.
Range of Levels
(dBA)
Communication Environment
70 to 80
Person-to-person communication with raised voice satisfactory 1 to 2 feet;
slightly difficult 3 to 6 feet. Telephone use difficult.
80 to 90
Person-to-person communication slightly difficult with raised voice 1 to 2
feet; slightly difficult with shouting 3 to 6 feet. Telephone use very
difficult.
Above 90
Person-to-person communication extremely difficult. Telephone use
unsatisfactory.
A2.3.3. Group Meeting, Study, and Rest and Relaxation Areas. Noise measurements made
to compare the noise environment in an area with these criteria should include internal and
external background noise. Acceptable levels are at Table A2.7. Note: Expected voice
represents the increase of voice level a speaker in a noisy field usually adopts. The
communicating voice level is the voice level a speaker can produce over the range of sound
levels shown when forced to communicate (achieve a 95 percent word score, with positive,
instantaneous feedback).
Table A2.7. Noise Levels for Group Meetings, Study, Rest and Relaxation*.
Range of Levels
(dBA)
Type of Space and Activities
34 to 45
Group gatherings to listen to speech and music; low background noise and
good hearing conditions required; sleeping.
45 to 55
Areas where some concentration and relaxed communication may be
desirable; reading rooms, sedentary relaxation; radio and television
listening.
55 to 65
Good communication conditions not essential; some distraction due to
external noise can be permitted; internal noise generation due to other
activities may be present.
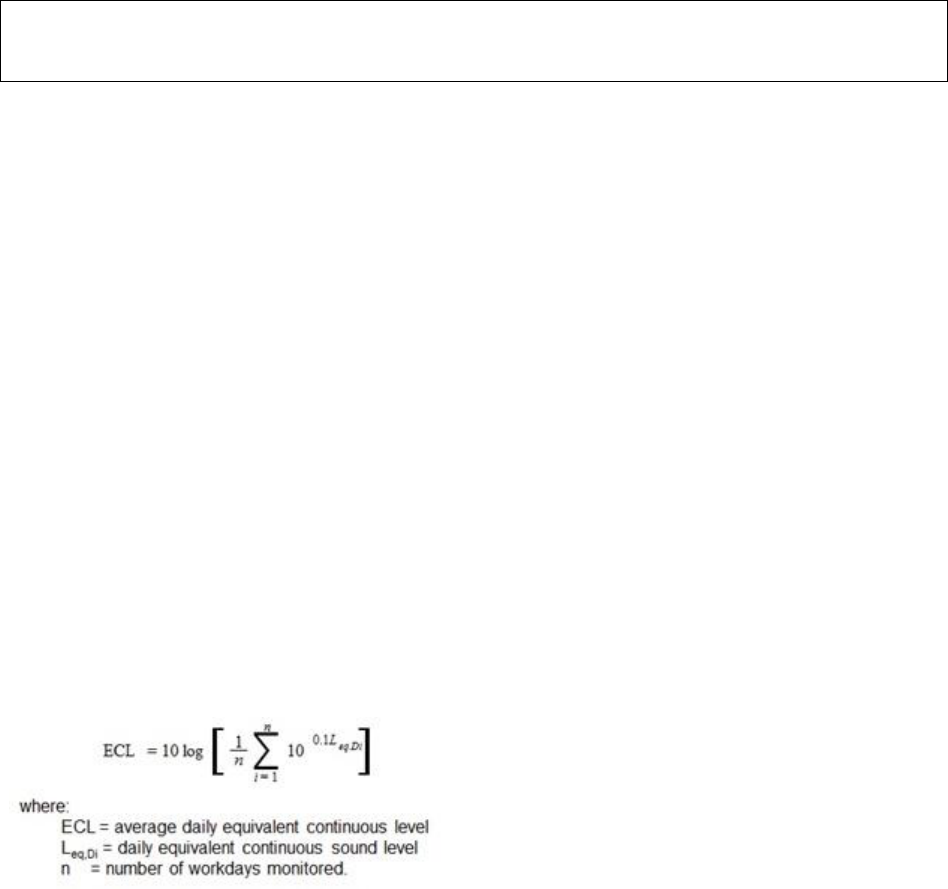
42 AFI48-127 26 FEBRUARY 2016
* Based on recommendations outlined in ANSI S12.65, American National Standard for Rating Noise with Respect
to Speech Interference.
A2.4. Music Exposure Criteria. Exposure to recreational music may lead to hearing damage;
two groups are typically affected: the employees (occupational exposure) and customers
(recreational exposure). The manager of each facility or activity where recreational exposure to
loud music may occur should post or issue precautionary warnings. BE personnel may provide
technical assistance in initial monitoring, interpreting results, and recommending controls.
A2.4.1. Employees. For employees who have occupational exposure to music, the noise
exposure limits and other provisions in this instruction apply as for any other group of
occupationally exposed employees.
A2.4.2. Customers. Entertainment planners and customers need some understanding of the
hazards associated with recreational exposure to loud music. Air Force occupational noise
exposure standards cannot be directly applied to recreational exposures. Assuming customer
exposure to loud music is generally limited to 2-hours, once per week, the music level should
not exceed an equivalent continuous level, Leq, of 94 dBA for any continuous 2-hour period
at any customer location. 94 dBA is a guideline and does not constitute a never to be
exceeded sound level. The intent is to allow music to be entertaining within reasonable and
safe limits.
A2.4.3. When multiple worker days are used to determine the average daily ECL for an
individual or group of individuals, the ECL can be used when formulating surveillance plans
and will be calculated according to the formula at Figure A2.5.
Figure A2.5. Calculating Average Daily Equivalent Continuous Level.
A2.5. Noise Surveys and Dosimetry.
A2.5.1. Frequency of Assessments. Potential noise hazards will be identified, assessed, and
controlled as an integral part of the assessments specified in AFPD 48-1, Aerospace
Medicine Enterprise, AFI 48-101, Aerospace Medicine Enterprise, and AFI 48-145.
Specifically, the health effects of noise will be evaluated as part of routine and special
assessments, and when operations change or new operations start. Additionally, assessments
are performed when specific requests address the potential for hazardous noise exposure or
evaluation of other types of requests show there to be potential noise hazards (OSHA 29 CFR
1910.95).
A2.5.1.1. An initial assessment will be conducted in all potentially hazardous noise
areas. Representative Leq,T noise level data will be collected for similar exposure group
(SEG) established IAW AFI 48-145 and AFMAN 48-146, Occupational and

AFI48-127 26 FEBRUARY 2016 43
Environmental Health Program Management, for all AF employees (military and
civilian) working in hazardous noise areas.
A2.5.1.2. An additional assessment should be accomplished within 30 days of any
change in operations affecting noise levels.
A2.5.1.3. When the noise exposures for a particular SEG are highly variable or not
clearly well above/below the OEEL, Leq,T evaluations will be accomplished IAW AFI
48-145 and AFMAN 48-146 to adequately characterize the noise hazard.
A2.5.2. Noise Hazard Survey. A generalized process sequence, coupled with specified
evaluation procedures, will be instituted to ensure a uniform approach to noise hazard
assessment. The objective is to determine whether noise exposures pose a significant risk to
the workers’ hearing. There are three phases in the health risk assessment process:
identification, analysis, and control.
A2.5.2.1. Identification. In this phase of health risk assessment the goal is to determine
whether a potential or existing exposure poses a health threat to a specified population
during a specified period and location. It is critical to understand the duties of the
populations and sub-populations. BE will become familiar with the processes being
performed in the workplace through firsthand observation, interviews with shop
personnel, review of existing assessment data, and epidemiological summaries completed
by PH. Potentially hazardous noise sources should be noted during this phase to identify
the need for further consideration in the analysis phase.
A2.5.2.2. Analysis. Three types of noise surveys are conducted to evaluate the noise
environment: the noise source survey, the worker exposure survey, and the hazardous
noise area survey. Data collection will be conducted when new processes are identified
or existing data is no longer current. Measurements will be made using equipment
conforming to the appropriate ANSI standard in the references. All noise data used to
characterize occupational exposures will be entered into DOEHRS-IH. Noise data
collected from 711 HPW/RHCB (Human Performance Wing/Battlespace Acoustics
Branch), or other independent source on behalf of the AF, will be provided to
USAFSAM/OE to disseminate to the BE career field for integration into DOEHRS-IH as
appropriate.
A2.5.3. Noise Source Survey. This survey is used to classify whether a particular noise
source output is equal to or exceeds the criterion level of 85 dBA and could present a
potential exposure hazard to workers. Sound level measurements will be made in accordance
with DoDI 6055.12, using A-weighting with slow response. If the source is determined to be
potentially hazardous, engineering controls will be considered before other control measures;
an octave band analysis may be necessary. Historical data should be applied to sources of
hazardous noise that have previously been well characterized, e.g., a generator for which the
sound pressure levels are adequately assessed. Hazardous noise sources will be labeled
where possible to warn operators of the need to wear hearing protection..
A2.5.4. Worker Exposure Survey. Where the potential to exceed the limits as discussed
under Noise Exposure Limits-Hearing exists, worker exposures will be evaluated by direct
measurements with noise dosimeters, or indirectly with noise exposure calculations specified
in Table A2.2.
44 AFI48-127 26 FEBRUARY 2016
A2.5.4.1. TWA noise levels will be determined for all AF workers working in hazardous
noise areas at least once and should be accomplished within 30 days of any change in
operations affecting noise levels. In circumstances such as high worker mobility,
significant variations in noise levels, representative personnel sampling will be
conducted.
A2.5.4.2. Impulsive noise and high level (>130 dB) continuous noise cannot be
accurately measured using traditional SLMs or dosimeters because special
instrumentation is required. If there is a request for additional information or impulsive
noise measurement, contact USAFSAM ESOH Service Center, 2510 Fifth Street,
WPAFB OH 45433, 1-888-232-3764, or AFRL/711 HPW/RHCB, 2610 Seventh Street,
WPAFB OH 45433.
A2.5.4.3. Worker noise exposure will be computed and reported regardless of any
attenuation provided by hearing protectors. However, workers should understand how
hearing protection devices effect their exposure levels.
A2.5.4.4. The decision to place an individual on the HCP will be based on the likelihood
of exposure at or exceeding 85 dBA as an 8-hour TWA. The following conditions should
be considered when estimating exposure for an individual or group of individuals
assigned to a SEG. These conditions are based on the assumption of no exposure to
hazardous noise in these environments:
A2.5.4.4.1. Number of days spent in classroom training;
A2.5.4.4.2. Number of days spent in administrative tasks, medical appointments
other duties, etc.;
A2.5.4.4.3. Number of days detailed to wing support not related to primary duty; or
A2.5.4.4.4. Number of days at formal training or temporary duty.
A2.5.5. Hazardous Noise Area Survey. These surveys are used to define work areas where
noise exposures are assumed hazardous based on routine operations. Hearing protection
requirements for these areas should be made clear to all personnel that might enter these
areas.
A2.5.5.1. These surveys can be used to define a work area enclosed by clear borders as a
hazardous noise area or to identify a hazardous noise zone around a certain piece of
equipment. When marking a hazardous noise zone around a piece of equipment, careful
consideration must be given to noise production variables and the equipment’s mobility.
A2.5.5.2. Instrumentation used for these surveys must meet or exceed requirements for
type 2 SLM as identified in ANSI Standard S1.4-1983 (R2006) and its most recent
revision. Instruments must have been subjected to a complete electro-acoustic calibration
based on manufacturers’ specifications before survey. Acoustical calibration must be
performed on the instruments before and after each day's measurements. The acoustical
calibrator must be accurate to within plus or minus one dB, and must have been subjected
to a complete electro-acoustic calibration.
A2.5.5.3. When personal noise dosimeters are used for worker exposure measurements,
they must integrate all sound levels from 80 dB to 130 dB. Dosimeters must meet or
exceed specifications in the latest approved ANSI Standard S1.25-1991 (R2007),

AFI48-127 26 FEBRUARY 2016 45
Specification for Personal Noise Dosimeters. AF components will use a time-intensity
exchange rate of 3 dB. Noise dosimeters are authorized for use in Sensitive
Compartmented Information Facilities, but local clearance will be obtained in advance
through the facility Sensitive Compartmented Information Security Officer.
A2.6. Noise Control. Engineering controls are the first choice to reduce hazardous noise
exposures existing in the workplace. Due to cost and design limitations associated with some
engineering control solutions, administrative controls and/or the use of personal protective
equipment may be necessary.
A2.6.1. Noise limit recommendations should be included as part of the acquisition process.
If the required equipment is not available within specified noise output limits, alternate
methods of noise control may be necessary. This may also be the case when noise levels
associated with existing equipment cannot be controlled cost effectively through engineering
solutions. To obtain a more detailed description or other examples of sound reduction
methods, consult the ESOH Service Center at website:
https://hpws.afrl.af.mil/dhp/OE/ESOHSC.
46 AFI48-127 26 FEBRUARY 2016
Attachment 3
CERTIFICATION AND EQUIPMENT STANDARDS
A3.1. Certification. Personnel performing audiograms as part of the USAF HCP will be trained
as Hearing Conservationists as established by the CAOHC. AF trained individuals may apply to
CAOHC to receive Certification. It is recommended that AF personnel obtain CAOHC-
approved HC training at either USAFSAM or DoD component, as it includes training on the
DOEHRS-HC software. Personnel who are CAOHC certified or receive training from a
CAOHC-approved civilian agency must contact USAFSAM to receive an AF Certification
number BEFORE performing audiometric testing because he/she will need to coordinate hands-
on training with the DOEHRS-HC software. Personnel who are CAOHC trained by a DoD
component will use the certification number issued by that Service. CAOHC-approved re-
certification is required at 5-year intervals for individuals active in hearing conservation testing.
A3.1.1. CAOHC trained Hearing Conservationists, are not trained or permitted to conduct
audiometric testing outside of requirements outlined in this instruction (i.e., audiograms for
diagnostic evaluations, school screenings, or hearing tests outside of the HCP with exception
to Sister Service readiness audiograms and threshold audiograms performed for the purpose
of separation history and physical exams).
A3.1.2. AF Certified Hearing Conservationists who perform audiograms must be responsible
to an audiologist, otolaryngologists, or other provider, OSHA 29 CFR 1910.95, (g)(3).
A3.2. Audiometric Equipment Standards. Audiometric testing done in support of the HCP
will be conducted with audiometers meeting the standards of ANSI S3.6-2010 (or current ANSI
standard). Audiometers must be DOEHRS compatible. Audiometric testing room requirements
are reflected in ANSI S3.1-1999 (R2008), Maximum Permissible Ambient Noise Levels for
Audiometric Test Rooms.
A3.2.1. Standardized HCP Audiometers. Routine pure tone air conduction testing is to be
accomplished with standardized HCP audiometers. DOEHRS-HC is the authorized system
for use in the HCP, and provides input into the DoD-wide Occupational Health databases.
Data from diagnostic clinical audiometers used by HCDC/HCC can be input manually.
Questions concerning the DOEHRS-HC system should be directed to the AF HCP Manager,
USAFSAM/PHR.
A3.2.2. Earphones. Only earphones meeting the requirements of ANSI Standard S3.6-2010,
or current ANSI standard, will be used in the AF HCP for screenings with DOEHRS-HC
software. Earphones must ONLY be used with the audiometer they were calibrated.
HCDC/HCC evaluations by audiologists only may use insert earphones that have been
appropriately calibrated by Biomedical Equipment Technicians or equivalent civilian
technicians. If the STS is due to collapsing canals, it is recommended to prevent the collapse
of the canal by placing a disposable HPD behind the pinna when using circumaural
earphones.
A3.3. Calibration, Testing, and Functional Checks. All audiometers and sound rooms must
be tested and calibrated before use in the HCP.
A3.3.1. Daily Functional Check. A daily functional check is required before each day’s use.
DOEHRS-HC software provides a functional check sequence. The examiner should listen to
AFI48-127 26 FEBRUARY 2016 47
all frequencies at various intensity levels. This general check of the machine and its function
will include listening for:
A3.3.1.1. Crackling sounds or changes in loudness while moving the cord.
A3.3.1.2. The presence of tones at all frequency settings.
A3.3.1.3. Presence of tones only in the appropriate headphone.
A3.3.1.4. Periods of silence while listening to the frequency and attenuation changes.
A3.3.2. Daily Calibration Check. Will be performed every day that hearing tests are
administered. DOEHRS-HC software provides a calibration check sequence. An examiner
who operates the audiometer must perform the calibration check in order to verify the system
is within calibration specifications. The calibration test subject can be an electroacoustic ear
or someone with known stable hearing levels, free of ENT problems, and not routinely
exposed to hazardous noise. Record the daily calibration results on the DD Form 2217,
Biological Audiometer Calibration Check. Note: Medical Equipment Repair Center
(MERC) will perform the equipment calibration when the equipment is not within
specifications according to the daily calibration check.
A3.3.2.1. If a change in threshold of more than plus or minus 5 dB at any frequency
(except 6,000 Hz), or more than plus or minus 10 dB at 6,000 Hz occurs, repeat the
calibration procedure. If the calibration standard is an electroacoustic ear, reset the
headphones and repeat the procedure. If the calibration test fails a second time, test a
person with known stable hearing thresholds.
A3.3.2.2. Headphones are calibrated with a specific audiometer; do not mix and match
headphones and audiometers that have not been calibrated together by Biomedical
Technicians. Out-of-calibration audiometers must not be used, checked by Biomedical
Technicians, and repaired or re-calibrated before being placed back in service.
A3.3.2.3. Document all activities on the DD Form 2217. A new DD Form 2217 must be
established when the audiometer is re-calibrated.
A3.3.3. Annual Acoustic Calibration. Audiometers used in the HCP will be acoustically
calibrated by Biomedical Equipment Technicians or appropriate provider of these services,
annually. The calibration date, taken from the hearing conservation forms, will be stored at
the DOEHRS-DR for 30 years.
A3.3.4. Exhaustive Calibration. Performed by Biomedical Equipment Technician every 2
years according to ANSI S3.6-2010 (or current ANSI standard). Test frequencies below 500
Hz and above 6,000 Hz may be omitted from this calibration for those audiometers used in
the HCP.
A3.4. DOEHRS-HC/DR. All hearing conservationists using DOEHRS-HC will have a DR
account.
A3.4.1. Prior to running a hearing test, previous tests must be inquired from the DR.
A3.4.1.1. If a previous reference audiogram has not been established, perform a
reference audiogram (on DD Form 2215) using a type 1 reason, prior to noise exposure.
48 AFI48-127 26 FEBRUARY 2016
A3.4.1.2. If any type of hearing test has been accomplished previously, an annual test
should be performed (on DD Form 2216).
A3.4.1.3. If a new reference is warranted, use a type 3 reason, reestablished after follow
up.
A3.4.1.4. If a member has separated from military service but will continue in civil
service in a noise-exposed job, a new reference will be established using a type 4 reason,
change in service component. This reason will also be used if the member changes from
civilian to uniformed military service.
A3.4.2. Hearing conservation technician or program manager must export data to the DR
every day that patients are seen using DOEHRS-HC data export function. Data must be
backed up to a secure device or network drive daily. When a new back up file is created,
previous files may be deleted. Only the most recent backup file is needed in case of a
computer crash. Exporting data to the DR is not the same as backing up the database. Both
must be accomplished.
AFI48-127 26 FEBRUARY 2016 49
Attachment 4
HEARING PROTECTION
A4.1. The use of personal hearing protectors to limit noise exposure is an interim protective
measure while engineering control measures are being explored, evaluated, and designed. Such
devices will constitute a permanent measure only if the BE determines, in coordination with the
workplace supervisor and the unit commander, that engineering controls are not technologically,
economically, or operationally feasible.
A4.2. Personal hearing protectors are provided at no cost to all AF personnel who work in
designated hazardous noise areas or operate noise-hazardous equipment.
A4.2.1. The worker’s organization will pay for the personal hearing protectors (including
custom molded hearing protection). However, if custom molded hearing protection is
required as determined by the MTF, the MTF provides the initial set and the worker’s
organization is responsible for replacements.
A4.2.2. The hearing protectors provided must be capable of attenuating worker noise
exposure below a TWA of 85 dBA. If hearing protectors do not provide sufficient
attenuation, further control of exposure will be necessary.
A4.2.3. An earplug carrying case will be made available by the owning organization (initial
issue and replacement based on normal wear and tear) for each set of pre-formed earplugs. It
will be provided at no cost to the AF personnel who work in designated hazardous noise
areas or operate noise-hazardous equipment. This case can also be used for hand-formed
earplugs. National stock numbers (NSN): Olive drab color, NSN 6515-01-100-1674 or
Navy blue color, NSN 6515-01-533-6168.
A4.3. Estimating Noise Attenuation for HPD. The noise attenuation provided by HPDs varies
between wearers, even when the wearers are highly skilled at fitting the HPDs to their ears.
A4.3.1. Multiple methods exist for selecting attenuation values; the recommended and most
preferred to least preferred methods are listed in Table A4.1 and A4.2. The AFRL
attenuation values along with other noise references can be found on the 711
th
portal/ESOH
Service Center at https://hpws.afrl.af.mil/dhp/OE/ESOHSC/.
Table A4.1. Preferred Methods for Selecting Attenuation Values for HPDs for Continuous
Noise.
1 - Most Preferred
AFRL ANSI measured values utilizing the ANSI S12.6
2
Other independent laboratories values utilizing the ANSI S12.6
3
Manufacturer values utilizing the ANSI S12.6
4 - Least Preferred
Manufacturer values utilizing ANSI S3.19 derated by 50% for earplugs
and 25% for earmuffs
50 AFI48-127 26 FEBRUARY 2016
Table A4.2. Preferred Methods for Selecting Attenuation Values for HPDs for Impulse
Noise.
1 - Most Preferred
AFRL ANSI measured values utilizing the ANSI S12.42
2
Other independent laboratories values utilizing the ANSI S12.42
3
Manufacturer values utilizing the ANSI S12.42
4 - Least Preferred
Manufacturer values utilizing ANSI S3.19 derated by 50% for earplugs
and 25% for earmuffs
A4.3.2. Methods for calculating effective noise levels at the ear. Apply hearing protector
attenuation data (mean minus two standard deviations) to noise levels. Note: The octave
band and NRR attenuation data used for calculation of the effective noise level under the
hearing protector shall be the mean minus two standard deviation attenuation data. This
ensures that approximately 98% (single tail normal distribution) of the users should achieve
the calculated attenuation value or more.
A4.3.2.1. The preferred method for applying hearing protector attenuation is the octave
band method. If the 8 hr TWA is greater than 92 dBA and the octave band method is not
being used, the ESOH Service Center must be contacted for guidance.
A4.3.2.2. A secondary method of calculating the effective noise level at the ear using the
NRR is allowable, but not preferred. A 7 dB correction factor will be applied to account
for the de-emphasis of low-frequency energy inherent to the A-weighting scale.
Following the 7 dB correction factor, an additional derating of 50% is required when
ANSI S3.19 NRR values are used. A4.3.2.2.1. When using ANSI S3.19 NRR values use
the following equation: Effective level at ear (dBA) = A-weighted level –
((NRR-7 dB) * 0.50)
A4.3.2.2.2. When using ANSI S12.6 NRR values use the following equation:
Effective level at ear (dBA) = A-weighted level – (NRR - 7 dB)
A4.4. Limits of Hearing Protection Performance. The maximum possible sound attenuation
provided by HPDs is limited by human body and bone conduction mechanisms. Even though a
particular device may provide outstanding values of noise attenuation, the actual noise reduction
may be less because the noise surrounding the head and body bypasses the hearing protector and
is transmitted through tissue and bone pathways to the inner ear.
A4.4.1. The term "double hearing protection" for earplug and earmuff combinations is
misleading. The attenuation provided from earplug and earmuff will be less than the sum of
their individual attenuation values. Never add individual HPD attenuation values to derive a
combination value. Consult the ESOH Service Center for information. If no data is
available, add 3 dB to the highest NRR of the plug or muff to estimate combined protective
rating.
A4.4.2. Wear of dual hearing protection in various conditions. When earmuffs are not worn
properly (i.e., airtight seal of the earmuff to the circumaural region surrounding the pinnae of
AFI48-127 26 FEBRUARY 2016 51
the ear) the amount of protection provided by the earmuff is greatly reduced and it is
impossible to determine how much protection the worker is receiving from the noise.
A4.4.3. For other conditions where earmuffs can be worn but an airtight seal cannot be
maintained (e.g., wearing of polar hood/balaclava for cold weather protection), then the
sound attenuation provided by the earmuffs in combination with earplugs and the protective
head gear will be assumed to equal the attenuation provided by the earplugs alone.
Administrative controls will be required to reduce the 8-hr TWA to below 85 dBA. Shop
supervisors will consult BE whenever such administrative controls are required.
A4.4.4. If earmuffs cannot be worn due to other PPE being worn around the head (e.g.,
respirator with airline) then ear-inserted single hearing protection must be used. If single
hearing protection does not provide enough protection to reduce the TWA 8-hr exposure
below 85 dBA then administrative controls, such as reduced time in the hazardous noise area,
are needed (assuming use of engineering controls has already been evaluated and is not
feasible). Shop supervisors will consult BE whenever such administrative controls are
required.
A4.5. Fitting and Dispensing Earplugs.
A4.5.1. PH will maintain a variety of earplugs, from at least two manufacturers and
including at least three sizes, as well as carrying cases. Individual units must purchase
earmuffs, disposable plugs, and other hearing protection variations approved by BE,
necessary to protect workers fully against hazardous noise.
A4.5.2. PH will accomplish initial earplug fitting. PH will fit and dispense pre-formed
earplugs and/or foam plugs at the time of the audiometric evaluation. At this time, PH will
assess the conditions (e.g., cold weather) in which the HPDs will be worn to ensure proper
wear for sufficient sound attenuation. Each ear will be individually fit with earplugs
(approximately 20 percent of the population requires a different size of earplug for each ear).
Workers unable to be properly fit with pre-molded or foam HPD will be referred by PH to an
AF audiologists or a certified licensed civilian audiologist for custom molded earplugs at AF
expense.
A4.5.3. Custom molded devices may be appropriate for special circumstances. Service band
members should be provided with pre-molded or custom molded musician’s earplugs, at their
unit’s expense. Only audiologists, otolaryngologists, and medical providers professionally
trained in custom earpiece fabrication may take impressions of the ear necessary to make the
custom molded earplugs.
A4.5.4. Workers may be fitted with pre-formed earplugs as determined by PH at the expense
of the AF. If workers request custom molded devices as a personal preference, the unit is not
obligated to pay for any additional examinations and the fabrication of specialized plugs.
However, if a unit chooses to purchase custom molded earplugs for their personnel, they
must consult with BE, PH, and the occupational medicine consultant who will provide
oversight of the brand/type selection, fitting, and monitoring of the custom devices. The
MTF may or may not provide resources to conduct the fitting of custom molded earplugs for
large numbers of personnel, depending on the availability of resources and personnel, and per
the MTF commander's approval.
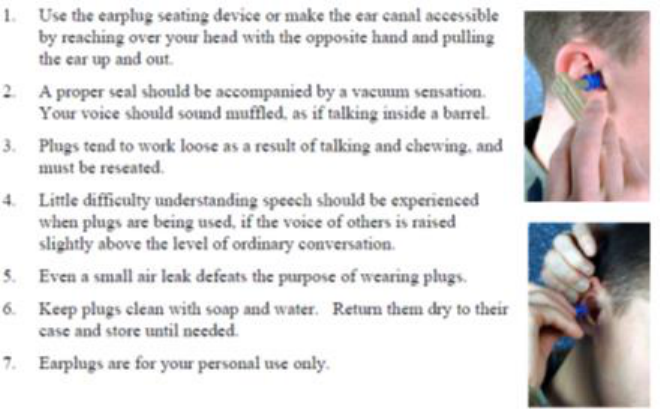
52 AFI48-127 26 FEBRUARY 2016
A4.5.5. PH will examine the fit and condition of all HPD (certified for use by BE) during the
annual audiogram, and whenever an effectiveness question exists (DoDI 6055.12 (6)(1)).
The worker will demonstrate proper fitting technique at the time of the audiogram. If a
worker cannot be adequately fit with the earplugs recommended by the BE, an audiologist
will determine an action plan that ensures the worker is adequately protected from
occupational hazardous noise.
A4.6. Types of Hearing Protective Devices.
A4.6.1. Insert Type Earplug. An insert earplug is designed to provide a seal with the ear
canal. There are three types of insert earplugs: premolded, formable, and custom molded
earplugs.
Figure A4.1. General earplug information.
A4.6.1.1. Premolded Earplugs (e.g., triple flange, Quattro). Premolded earplugs are
pliable devices of fixed proportions. Personnel fitting and dispensing earplugs will train
users on proper insertion, wear, and hygiene. They are reusable, but may deteriorate and
need replacement. The earplugs should be discarded if they become brittle or torn, or if
routine cleaning cannot remove debris.
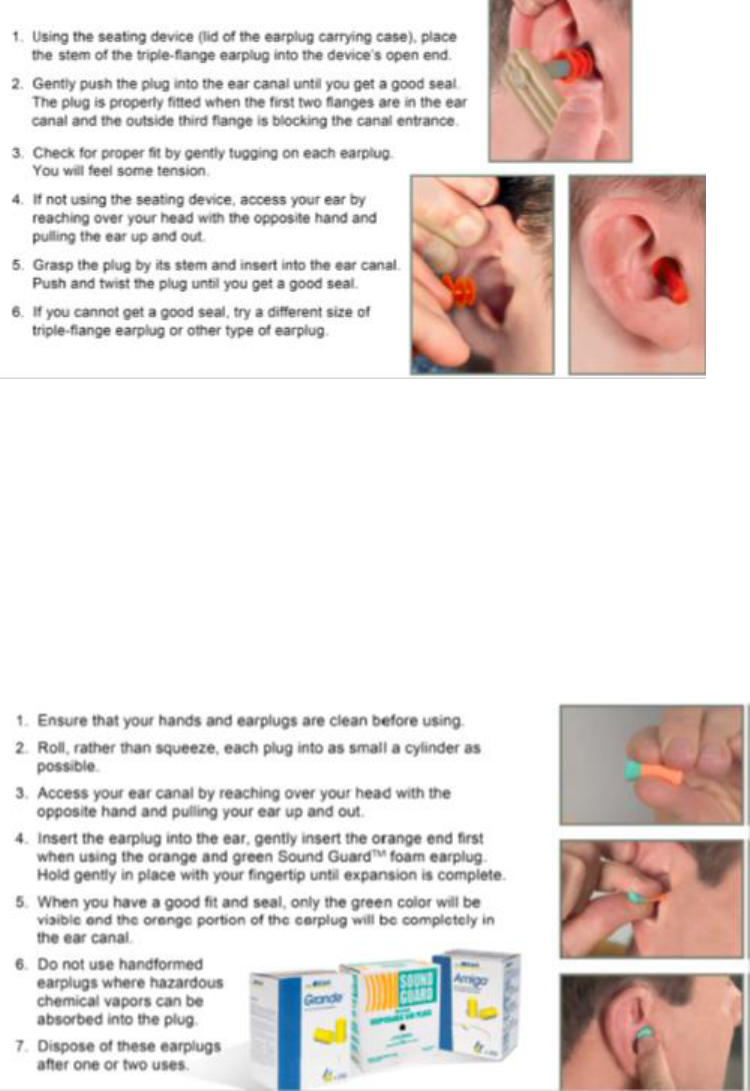
AFI48-127 26 FEBRUARY 2016 53
Figure A4.2. Instructions for Triple-Flange Earplugs.
A4.6.1.2. Formable Earplugs (e.g., foam). Formable earplugs are made of material that,
after compression and insertion, expands to form a seal in the ear canal. When properly
inserted, they provide noise attenuation values that are similar to those from correctly
fitted premolded earplugs. Formable earplugs are usually considered disposable, and
therefore are more expensive for long-term routine use. Individual units may procure
approved formable earplugs. Each earplug must be held in place while it expands enough
to remain firmly seated. These earplugs may be washed and reused, but should be
replaced after five uses or when they no longer form an airtight seal when properly
inserted.
Figure A4.3. Instructions for Foam (Hand formed) Earplugs.
A4.6.1.3. Custom Molded Earplugs. A small percentage of the AF population cannot be
fitted, as determined by the MTF, with standard premolded or formable earplugs.
Custom molded earplugs are made to fit the exact size and shape of an individual's ear
canal. AF Band members are authorized to obtain custom molded musician's earplugs
without medical determination. All individuals needing custom molded earplugs will be
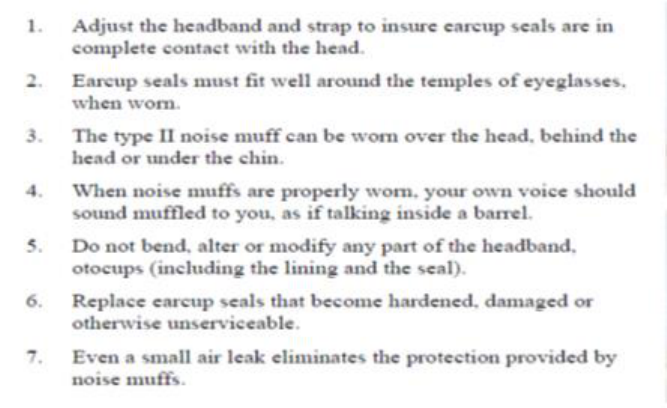
54 AFI48-127 26 FEBRUARY 2016
referred by Public Health to an AF audiologist or licensed civilian audiologist. The
selected custom molded earplug must be reviewed by BE to confirm it meets the
attenuation requirements of that individual’s workplace.
A4.6.2. Earmuffs. Earmuffs are devices worn around the ear (circumaural) to reduce the
noise reaching the ear. Their effectiveness depends on a tight seal between the cushion and
head.
Figure A4.4. General Information on Earmuffs (eg, noise muffs).
A4.6.2.1. Earmuffs and other HPD with input capacity, such as for music players or
built-in radios designed for recreational listening will not be used with or as protectors.
Any HPD with input capacity must be approved for use by 711 HPW/RHCB to evaluate
the device to confirm the level of output is not harmful, or limit to non-harmful levels.
Consult installation BE for more information.
A4.6.2.2. Communication Earmuff's (Electroacoustic Devices). Personnel who must
communicate in the presence of intense noise use these devices, as determined by BE.
They are fitted with earmuffs and, if needed, a noise-shielding or noise cancelling
microphone so voice communications can be achieved during various operations. Noise
exposure limits may be exceeded by the combination of external noise plus voice. Sound
levels produced by communication devices only need to be measured if they represent the
primary noise exposure; communications are considered the primary noise source when
background noise levels are 85 dBA or less.
A4.6.2.3. Combination Communications Earmuff and Earplug. When extremely high
noise levels are present and attenuation of communication earmuffs does not allow
enough exposure time to complete the mission, earplugs can be worn in addition to the
earmuffs. Custom molded earplugs can be made under the supervision of an audiologist.
This combination of protection should provide a longer allowable exposure time for
mission completion. Information on modifications of earmuffs and fabrication of custom
molded earplugs can be obtained from USAFSAM/PHR and ESOH Service Center.
AFI48-127 26 FEBRUARY 2016 55
A4.6.3. Active Noise Reduction (ANR) hearing protection may not be appropriate for all
industrial and/or military environments. Before employing ANR hearing protection, contact
ESOH Service Center to assist in determining the appropriateness and feasibility of ANR
applications. Additionally, ANR device data used in the HCP should be IAW the most
current ANSI standards, for measuring passive and active attenuation.
A4.6.4. Communication headsets, typically used by flight crew as hearing protection during
engine start up, are designed to provide hearing protection and simultaneous communication
capability and are appropriate in some environments. Contact ESOH Service Center to assist
in determining the appropriateness and feasibility of these applications. Additionally,
communication measurements should be IAW with the most current ANSI standard.
A4.6.5. Flight Helmets. Flight helmets used during ground or airborne operations provide
varying degrees of protection from noise. The ear enclosures in these devices determine the
degree of protection achieved. Generally, the amount of protection provided, primarily at
frequencies below 1,000 Hz, varies with the condition of the ear enclosures and the acoustic
seal. Headset ear enclosures and ear cushions must be maintained in good repair.
A4.6.6. Hearing aids are not hearing protectors. Certain hearing aids or surgically implanted
devices may be used with over-the-ear hearing protectors after evaluation and approval by an
audiologist or otolaryngologist. If approved, the worker should be closely scrutinized on
evaluation to determine STS after occupational noise exposure.
A4.7. Education and Training on Proper Use, Care, and Maintenance of HPDs.
A4.7.1. PH will train personnel on the proper use and care of HPD at the time of audiometric
testing. Personnel requiring earmuffs (in addition to earplugs) will be informed of this
requirement and educated on the importance of using adequate protection.
A4.7.2. Supervisors will instruct users on proper use and care of HPDs in the workplace as
part of the annual training program.
A4.7.3. Reusable earplugs or formable devices should be washed in lukewarm water with
hand soap, rinsed in clean water, and dried thoroughly. Wet or damp earplugs should not be
worn or placed in their containers. Cleaning should be done as needed.
A4.7.4. Earmuff seals should be kept clean. The plastic or foam cushions may be cleaned in
the same way as earplugs, but the inside of the muff should not get wet. When not in use,
earmuffs should be placed in open air to allow moisture that may have been absorbed into the
cups to evaporate. Earmuff seals should be replaced as needed.
A4.7.5. Anyone having difficulty in wearing hearing protection (i.e., irritation of the ear
canal(s) or pain) should immediately report this to their supervisor. The supervisor should
remove the worker from exposure to hazardous noise and contact their provider or PH.
56 AFI48-127 26 FEBRUARY 2016
Attachment 5
FITNESS AND RISK EVALUATIONS
A5.1. Personnel who cannot perform essential job functions, and/or pose a safety risk to
themselves or others, because of a medical condition, will be evaluated for fitness and risk. The
fitness and risk evaluation may be requested by the medical provider or by line management.
Clinical evaluations by either HCDC/HCC, other DoD, VA or network audiologist are required
as part of the fitness and risk evaluation. Personnel will be considered for a fitness and risk
evaluation if they demonstrate any of the following:
A5.1.1. Show a second PTS in either ear.
A5.1.2. Exceed the H-1 profile and work in a hazardous noise area.
A5.1.3. Complain of not hearing/understanding spoken communications, auditory cues or
signals.
A5.1.4. Exhibit behavior resulting in invalid or unreliable audiograms (Failure to obtain
accurate audiometric test data should result in a worker being removed from all hazardous
noise environments due to an inability to accurately monitor hearing).
A5.1.5. Exhibit behaviors that call into direct question the ability to work in the assigned
job.
A5.1.6. Cannot be fit with HPDs.
A5.2. Flying and other special operational duty personnel who meet the criteria above or exceed
hearing standards for their flying class will be evaluated as directed in AFI 48-123. Note: A
fitness and risk evaluation is performed as part of the waiver process for flying and other special
operational duty personnel who exceed hearing standards IAW the Medical Standards Directory.
If there has not been a PTS since waiver approval, an additional fitness and risk evaluation is not
warranted. However, if there has been a PTS since waiver approval, consult a flight surgeon for
initiating a fitness and risk evaluation.
A5.3. For non-flying personnel, the provider initiates the fitness and risk evaluation in
coordination with the installation level HCPM.
A5.3.1. The provider must address clinical status and job safety in the Reason(s) For
Request section of AF Form 1754. The provider may include a job capability assessment in
the informed medical recommendation.
A5.3.2. The provider will perform a clinical examination. As a minimum, the routine
clinical exam (AF Form 1753, Section II) will be performed. If other medical conditions
affect the person’s ability to perform the job capably or safely, they will be addressed in the
clinical examination.
A5.4. The Job Capability and Safety Analysis.
A5.4.1. Base Personnel Flight must prepare a list, using the AF Form 1754, Part 2, of the
minimum essential tasks and auditory requirements a worker must have for job qualification.
A5.4.2. Installation level HCPM completes the Job Capability Survey, using the AF Form
1754, Part 3. HCPM interviews the worker, visits the workplace, and for each task identified
AFI48-127 26 FEBRUARY 2016 57
by the appointing official makes a judgment if the worker will be able to capably perform the
task.
A5.4.3. When requested by the medical provider, the safety representative in conjunction
with the shop supervisor will analyze job safety, complete AF Form 1754, Part 4, and return
the form to the medical provider. The Job Capability Survey (Part 3) and the Job Safety
Analysis (Part 4) should be performed at the same time.
A5.4.3.1. In consultation with BE and PH, Safety officials interview the worker, visit the
workplace, and for each task identified by the appointing official, make a judgment as to
whether the worker should be able to reasonably perform the task without endangering
themselves or others.
A5.4.3.2. The safety analysis should address, but is not limited to, the following
conditions:
A5.4.3.2.1. Does the worker perform tasks alone or in-groups?
A5.4.3.2.2. If group tasks are required, are visual cues available?
A5.4.3.2.3. Does the worker need to communicate to perform tasks?
A5.4.3.2.4. Do potential hazard signals exist that the worker needs to hear (forklifts,
special machinery, announcements, etc.)?
A5.4.3.2.5. Do the job tasks include confined space entry?
A5.5. Medical Determinations and Recommendations. The medical provider will only make
a recommendation whether the worker will be able to capably perform the task. The appointing
official/commander makes the final decision.
A5.5.1. To assist managers in making employment and placement decisions, medical
recommendations will be one of the following:
A5.5.1.1. Worker meets medical requirements of the position.
A5.5.1.2. Worker meets medical requirements with an accommodation or restriction.
(List recommended accommodations or restrictions and the expected therapeutic or risk
avoiding benefit considering risk management decision-making process).
A5.5.1.3. Worker is not fit to perform essential tasks, will pose an undue risk to
themselves or others, or fails to meet medical requirements for the job. The medical
provider must include reasonable justification for recommendations.
A5.5.2. A determination of hearing profile might also be necessary IAW AFI 48-123. AF
Form 422 and H-1 profile designation are not appropriate for civilian employees. Hearing
profiles are not appropriate for decisions concerning disposition and/or disqualification.
Individual worker determinations are made on a case-by-case basis as outlined by the Fitness
for Duty Evaluation.
A5.5.3. The provider may assume a worker meets the minimum medical qualifications to
perform a job in a hazardous noise environment if one of the following conditions is true:
58 AFI48-127 26 FEBRUARY 2016
A5.5.3.1. Worker has an H-1 profile, can wear standard HPDs, and does not report
difficulty hearing and understanding routine spoken communications, auditory cues, or
signals.
A5.5.3.2. Worker has undergone a previous fitness and risk evaluation, hearing
thresholds have not changed significantly (no STS compared to most current reference),
medical condition that may affect job performance in a hazardous noise job has remained
stable; and the worker’s supervisor has not expressed any new concerns.
A5.5.4. The medical recommendation for placement or continuation in a noise-hazardous
job will include the following statement on the AF Form 422, Notification of Air Force
Member’s Qualification Status, or locally derived return to duty memo, “This worker meets
medical standards to work as a [insert job title and occupation code] in [insert shop name
and number].” If restrictions or accommodations are recommended, they should be listed on
AF Form 422, or locally derived return to duty memo, along with the expected risk-reducing
or therapeutic benefit.
A5.5.5. A disqualifying medical determination is warranted if:
A5.5.5.1. Allowing the worker to perform the job would exacerbate a preexisting
medical condition and no reasonable accommodation would enable the worker to perform
essential functions of the job without exacerbation or further damage to the known
preexisting medical condition.
A5.5.5.2. Allowing the worker to perform the job would endanger their safety, the safety
and security of other workers, or the public.
A5.5.5.3. The worker fails to meet a valid medical standard or physical requirement for
placement in the position.
A5.5.5.4. The worker determined to be medically disqualified because of reasons above
must be individually evaluated.
A5.5.6. A summary of the fitness and risk evaluation will be prepared, using an AF Form
422, or locally derived return to duty memo, by the provider and will contain the following
minimum information:
A5.5.6.1. Reason for the fitness and risk evaluation.
A5.5.6.2. Clinical status (determination of whether a medical condition is temporary or
permanent, and has reached maximum medical benefit).
A5.5.6.3. Safety assessment results.
A5.5.6.4. Recommendations for accommodations and (or) restrictions in the particular
job.
A5.5.7. The completed AF Form 1754 will be forwarded to PH who will then forward to the
appropriate medical record authority for inclusion in the member’s medical record (T-2).
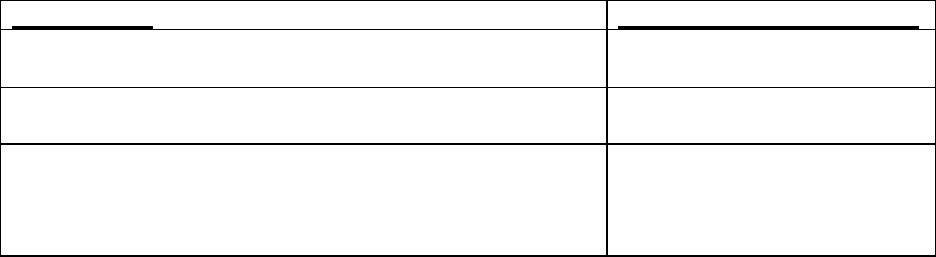
AFI48-127 26 FEBRUARY 2016 59
Attachment 6
HEARING CONSERVATION DIAGNOSTIC CENTERS (HCDC)/HEARING
CONSERVATION CENTERS (HCC) AND REFERRAL CRITERIA
A6.1. An HCDC is located at an AF medical treatment facility. It provides a wide range of
diagnostics and treatments in support of clinical referrals for hearing conservation, and provides
services to all other persons authorized medical care by AFI 41-210, Tricare Operations and
Patient Administration Functions.
A6.2. An HCC is a center located at an AFMC installation that provides direct support for
referrals under the HCP.
A6.3. In order to provide support, HCDCs and HCCs must consist of an audiologist and support
staff. Evaluations by certified military or state licensed civilian audiologists are permitted. All
evaluations by non-DoD audiologists will be reviewed by the regional HCDC or HCC.
A6.3.1. The HCDC and HCC provide consultation and overview of referrals, so the
management and disposition of patients meet current AF standards. Guidance can be via
“standing order” or record review. Record reviews can be accomplished by fax, or encrypted
email, if Health Insurance Portability and Accountability Act (HIPAA) compliant. The
reviewing audiologist must create an encounter in the electronic medical record to document
that a record review has taken place and provide a patient disposition to include
recommendations for reference audiogram re-establishment, return to duty or restrictions,
OSHA reporting requirements and any follow-up required.
A6.3.2. At a minimum, testing capabilities will include diagnostic audiometer equipment
sufficient to complete a full comprehensive hearing exam, a full range of immittance,
electrophysiological, and otoacoustic emissions equipment.
A6.4. Referral Criteria. Medical providers may validate a PTS, but the Occupational Health
Consultant or audiologist may be consulted to review problem audiograms to determine if further
evaluation is required before re-establishing a reference audiogram. If the medical provider
determines no further evaluation is required, then proper documentation in the Electronic Health
Record must be provided to explain why no further follow-up was required. Medical providers
should use Table A6.1. to determine if a referral is recommended. Note: Aircrew members who
fail to meet the requirements for continued flight duty will be evaluated as specified in AFI 48-
123.
Table A6.1. Referral Criteria.
CONDITION
RECOMMENDED ACTION
On pre-placement, have a hearing profile exceeding H-1
(reference the Medical Standards Directory).
Fitness and Risk Evaluation*
For medical reasons may not be able to perform the job
capably or safely in a noise hazard environment.
Fitness and Risk Evaluation*
Have a PTS following required Noise Free evaluation.
Audiologists and providers are permitted by OSHA
regulations to reestablish reference audiograms without
HCDC/HCC referrals, with appropriate electronic
Referral to HCDC/HCC
60 AFI48-127 26 FEBRUARY 2016
documentation of non-referral rationale.
Are unable to wear standard hearing protective devices.
Referral to HCDC/HCC
Complain of inability to correctly hear or understand routine
spoken communications, auditory cues, and signals.
Referral to HCDC/HCC
Need special hearing skills and complain of hearing
problems. (For example, Morse or voice-intercept
operators, air traffic controllers, etc.)
Referral to HCDC/HCC
Are unable to test using standard procedures or equipment.
Referral to HCDC/HCC
Have a 40 dB or greater difference between ears at any
frequency. (Requires masked audiogram)
Referral to HCDC/HCC
Have asymmetric hearing loss greater than or equal to 25 dB
difference between the left and right ears at any two
consecutive frequencies.
Referral to HCDC/HCC
(Once referral is completed
annual follow-up not required
if asymmetry is stable)
Exhibits behavior resulting in invalid or unreliable test
results suggesting an exaggerated hearing loss or a problem
unrelated to a known physical illness or disease.
Referral to HCDC/HCC
Meet other referral criteria as determined by the consulting
audiologist or program manager.
Referral to HCDC/HCC
* Requires clinical evaluation by audiologist
A6.5. Processing Patient Referrals. Medical referrals for STS should be completed as quickly
as possible upon completion of the follow-up testing process and are the responsibility of the
medical facility, and will be completed within the designated referral timeframe.
A6.5.1. Providers will complete an electronic referral to Audiology for further evaluation,
indicating the reason for the referral and request of care, and send the patient to the
appropriate administrative MTF function to schedule the referral appointment. The MTF
scheduler arranges appointment and travel orders, and notifies the patient, the patient’s
supervisor, PH, and the referring provider of the date, time, and location of the appointment.
The patient’s medical record and referral information must be available to the HCDC/HCC
or Occupational Health consultant at the time of the examination. The provider may use the
DOEHRS-HC generated SF 600e, DOEHRS-HC Hearing Loss Referral, or the AF Form
1672, Hearing Conservation Diagnostic/Center Referral, as another option to submit the
referral.
A6.5.2. When the local MTF does not have the capability to provide an examination (or a
portion of the exam) for the civilian employee, the MTF may arrange to have the
examination in the civilian sector (non-DoD) healthcare community after receiving
authorization from the employee’s unit commander. The employee’s unit commander must
also authorize payment for the examination. Payment is made from the same appropriation
that funds the employee’s salary IAW AFI 65-601v1, Budget Guidance and Procedures. In
cases where a civilian worker requests an audiological evaluation for other than an
occupationally related condition, i.e. hearing aid assessment, the employee will pay for the
evaluation at a civilian establishment and any associated costs (e.g., travel, etc.).
AFI48-127 26 FEBRUARY 2016 61
A6.5.3. In cases where HCDC/HCC audiology availability, travel restrictions or finances
prohibit referral to an HCDC/HCC, the patient should be referred to a licensed and/or
certified civilian audiologist. Providers may consult with the AF/SG Audiology Consultant
on military or civilian audiology service selections and results interpretation. An AF
audiologist is required to review/consult on all audiometric evaluations performed by non-
DoD audiologists. See Paragraph 2.20.14.6.1 for a list of requirements.
A6.5.4. The HCDC/HCC audiologist will enter into the electronic medical record the
audiological evaluation results and patient disposition to include recommendations for
reference audiogram re-establishment, return to duty or restrictions, OSHA reporting
requirements and any follow-up required. The provider may complete and upload the
DOEHRS-HC generated SF 600e or AF Form 1672 with results and associated disposition
into the electronic medical record.
A6.6. HCDC/HCC Listing.
A6.6.1. 779 AMDS/SGPE, 1050 West Perimeter Rd., Joint Base Andrews, MD 20762
A6.6.2. 31 MDOS/SGOV, Unit 6180 Box 245, Aviano AB, APO AE 09604
A6.6.3. 96 AMDS/SGPQ, 307 Boatner Rd. Bldg 2825, Eglin AFB, FL 32542-1282
A6.6.4. 673 MSGS/SGOSLA, 5955 Zeamer Ave, Joint Base Elmendorf-Richardson, AK
99506-3700
A6.6.5. 75 AMDS/SGPQ, 7238 6th Street, Hill AFB, UT 84056-5012
A6.6.6. 81 MSGS/SGPQ, 301 Fisher St., Room GE240, Keesler AFB, MS 39534
A6.6.7. 59 SGC/SGCXA, 2200 Bergquist Dr. Ste.1, Joint Base San Antonio, TX 78236-
9908
A6.6.8. 48 MSGS/SGCU, Unit 5210 Box 230, RAF Lakenheath, APO AE 09461-0230
A6.6.9. 633 AMDS/SGSE, 77 Nealy Ave, Joint Base Langley-Eustis, VA 23665-2080
A6.6.10. 6 AMDS/SGPQ, 3250 Zemke Ave., MacDill AFB, FL 33621-1607
A6.6.11. 99 MSGS/SGCX, 4700 N. Las Vegas Blvd., Nellis AFB, Las Vegas, NV 89191
A6.6.12. 55 MDOS/SGOSLA, 2501 Capehart Rd. Offutt AFB, NE 68133-2160
A6.6.13. 78 AMDS/SGPQ, 655 7th Street Bldg. 207, Robins AFB, GA, 31098-2227
A6.6.14. 52 MDOS/SGOT, Unit 3690 Bldg 61, Spangdahlem AB, APO AE 09123-3690
A6.6.15. 72 AMDS/SGPOA, 8941 Entrance Rd., Bldg 3334, Tinker AFB, OK 73145-5300
A6.6.16. 60 AMDS/SGCPQ, 101 Bodin Circle, Travis AFB, CA 94535-1880
A6.6.17. 10 MDOS/SGOA, 4102 Pinion Drive, USAF Academy, CO 80840-4000
A6.6.18. 88 AMDS/SGPQ, 2325 Fifth Street, Bldg 675 Area B, Wright-Patterson AFB, OH
45433-7021
A6.6.19. 374 AMDS/SGPO, Unit 5227 Bldg 440, Yokota AB, APO, AP 96328-5227
A6.6.20. 86 MDS (Landstuhl Regional Medical Center), Attn: Audiology Clinic, CMR 402,
APO AE 09180
62 AFI48-127 26 FEBRUARY 2016
Attachment 7
OWCP HEARING LOSS MEDICAL REQUIREMENTS AS PARAPHRASED FROM
DOL OWCP HEARING LOSS SECTION INSTRUCTIONS
A7.1. The report submitted must include the results of an otological (ENT) exam, conducted by
a provider, and the results of an audiological exam administered in a sound-treated booth. Please
forward both the ENT report and the audiological evaluation to the office designated to handle
worker compensation claims (e.g., Civilian Personnel Office). Bills may only be paid when we
have received the ENT report and the audiological evaluation.
A7.1.1. The report of the provider's ENT examination must include:
A7.1.1.1. The date and hour of examination;
A7.1.1.2. The date and hour of the claimant's last exposure to employment related noise;
A7.1.1.3. A detailed and relevant medical history;
A7.1.1.4. The provider's reasoned opinion concerning the etiology of any indicated
hearing loss and, specifically, its relationship to the claimant's occupational noise-
exposure history;
A7.1.1.5. The provider's recommendations for treatment, including the need for a
hearing aid; and, the provider's original signature.
A7.1.2. The report of the audiological evaluation must include:
A7.1.2.1. An authenticated, legible, and dated audiogram consisting of pure tone air
conduction threshold from 250 to 8,000 Hz, including 3,000 Hz, and bone conduction
thresholds from 250 to 4,000 Hz, also including 3,000 Hz;
A7.1.2.2. The results of speech reception threshold (SRT) and speech discrimination
testing, including stimuli and method of presentation (SRT and pure tone average (PTA)
should agree within ± 10 dB);
A7.1.2.3. The results of an impedance test battery, including tympanometry and
stapedial reflex threshold measurements;
A7.1.2.4. The standard and date of last electronic calibration, and the name of the person
who performed the calibration, (our procedures require that the date of last electronic
calibration be within 1 year of the date of examination) for each instrument used;
A7.1.2.5. A statement regarding the reliability of the audiological evaluation (if
questionable, administer additional tests so that reliable conventional audiometric
responses will be obtained); and, a statement indicating that the claimant was removed
from any exposure prior to your examination.
